Maternal health inequities persist. Can digital tools be part of the solution?
Digital tools can empower the maternal health ecosystem, but there is a need for better cultural tailoring and increased ease of use.
Kulleni Gebreyes
Heather Nelson
Margaret Punch
Jay Bhatt
Mani Keita
Christine Chang
Maternal health is a worldwide issue, and the United States is no exception. In fact, it has the highest maternal mortality rate of all developed countries.1 Racial disparities exist across all US income and education levels, with maternal mortality among Black women occurring three times more often than among White women,2 due to inequities in access and care.3 The maternal health ecosystem can do more than just ensuring that women survive pregnancy.4 However, substantial challenges remain in identifying and addressing patient needs efficiently and equitably. While not a silver bullet, digitally enabled care and tools could help increase access to and utilization of timely and tailored care.5
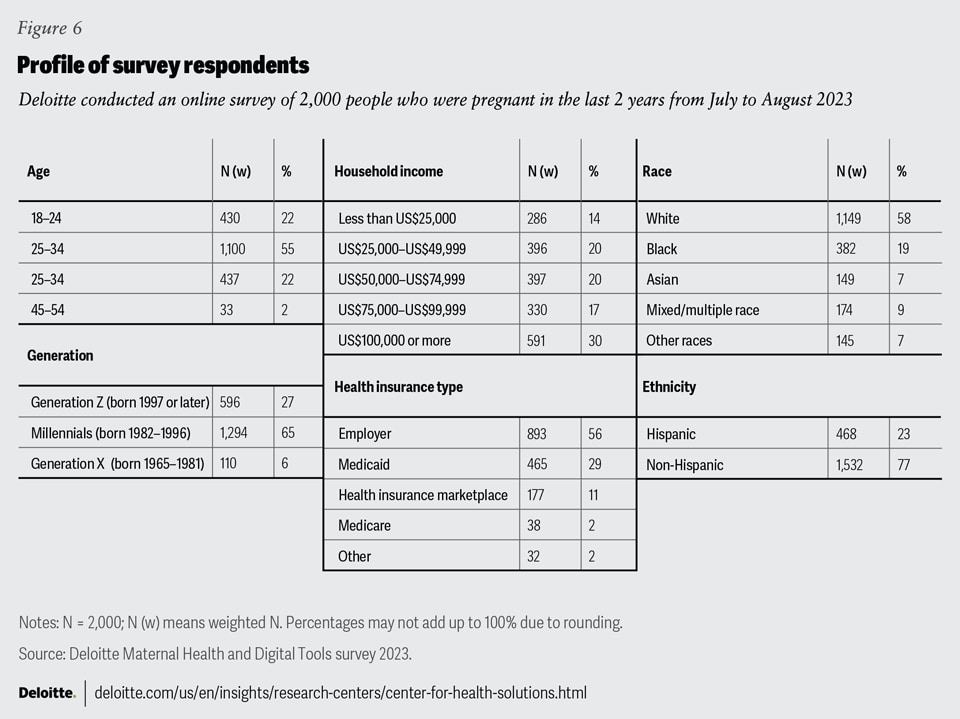
To understand how digital tools can be helpful and how maternal health–focused organizations are using technology and digital tools to improve health care disparities and access for people across the pregnancy journey, the Deloitte Center for Health Solutions conducted a survey in the United States in July and August 2023 of 2,000 people who were pregnant in the previous two years and interviewed a wide range of stakeholders (see “Appendix: Study methodology, respondent profiles, and data analysis” for more information). We found that digital tools could boost maternal health empowerment, with more than 70% of respondents using digital tools to manage specific health needs, going beyond accessing health care and receiving or sending communication.
However, Black, mixed-race, and Hispanic respondents were twice as likely as White respondents to say that digital tools for maternal health did not meet their personal needs or align with their cultural backgrounds. This indicates that, as US health care providers work to activate a maternal health ecosystem that improves pregnancy and child health outcomes, it’s important to understand people’s unique experiences and needs when using digital tools to support maternal health and equity.
Digital tools could improve access to care and help manage maternal health needs
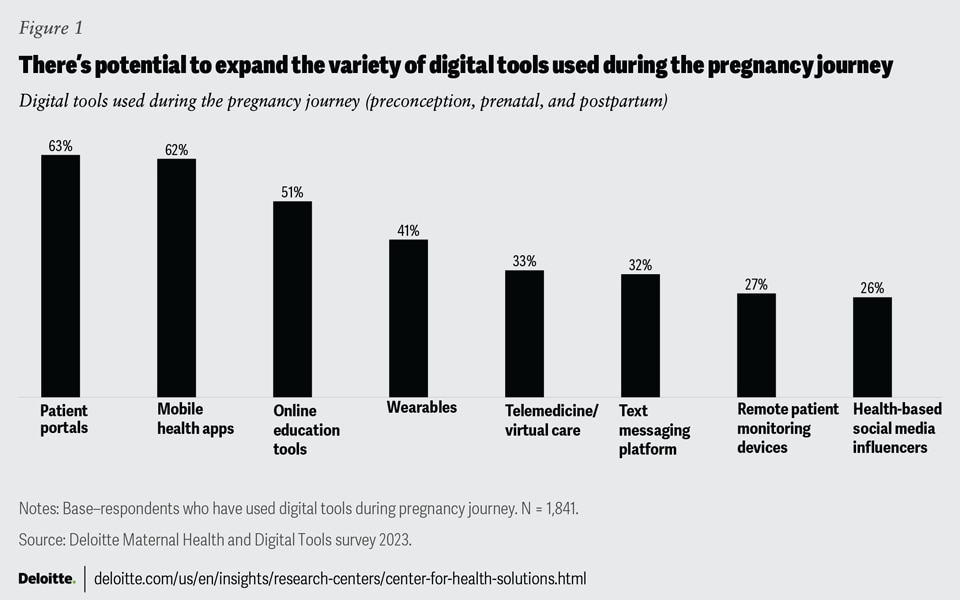
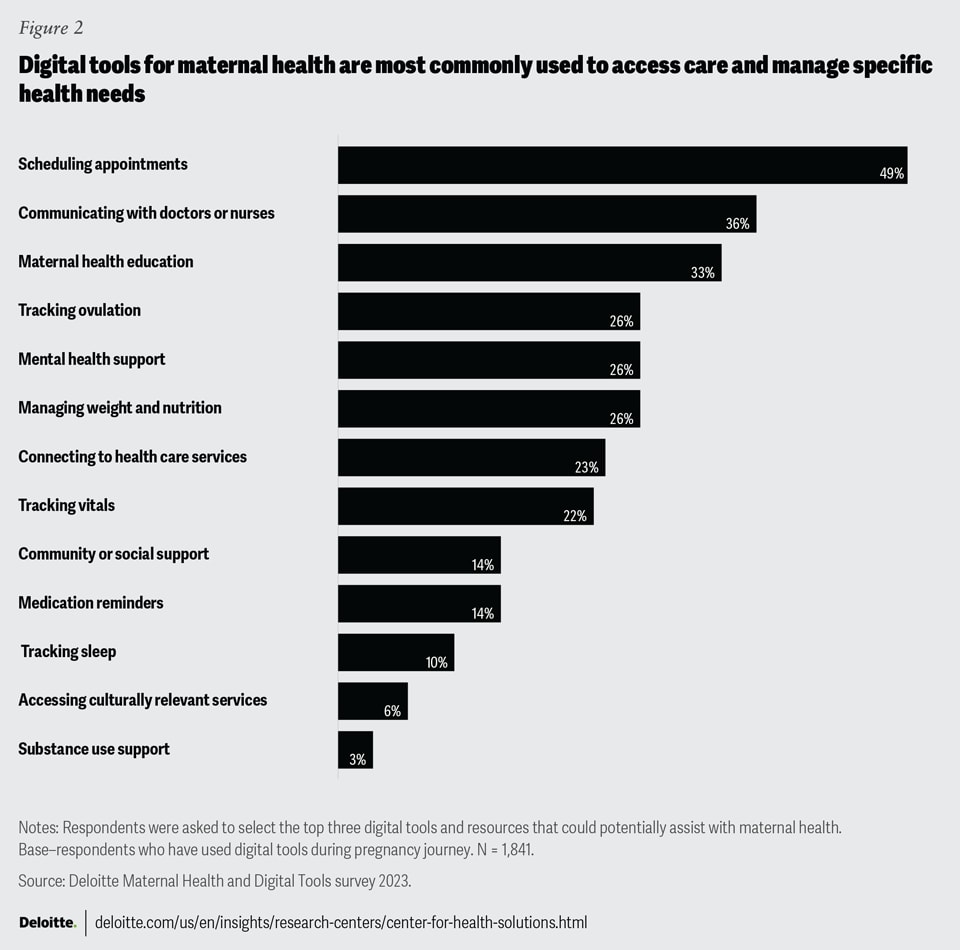
Digital tools for maternal health can act as a gateway to enhance accessibility to care teams and health services, and to aid patients in addressing specific needs. According to the survey findings, patients of all racial groups are using patient portals and mobile health apps most frequently across the pregnancy journey (figure 1). Nearly half of the respondents use digital tools to access care, with 49% using the tools to schedule appointments and 36% using them to communicate with their care team (figure 2).
Patient portals, online scheduling platforms, and communication tools are the bare minimum that should be provided to patients to access care. However, a deeper look shows that using digital tools can help patients meet more specific needs when it comes to getting the care they need. According to the survey, 77% of respondents are using digital tools to monitor reproductive cycles, manage weight and nutrition, support mental health, and educate themselves on maternal health.
Through our focus group and interviews, we found that, overall, health care providers are already using some digital tools like telehealth but are interested in venturing further. Advancements like virtual doula care have been shown to educate patients on maternal warning signs, help manage mental health, provide emotional support during pregnancy, and ultimately reduce the need for a cesarean delivery.6 Boosting health systems’ proficiency in using digital tools for maternal health is important to effectively address patients’ unique needs. One large health system is using an artificial intelligence–enabled pregnancy chatbot that provides a virtual safety net by sending alerts to the care management team depending on patient responses and data.7
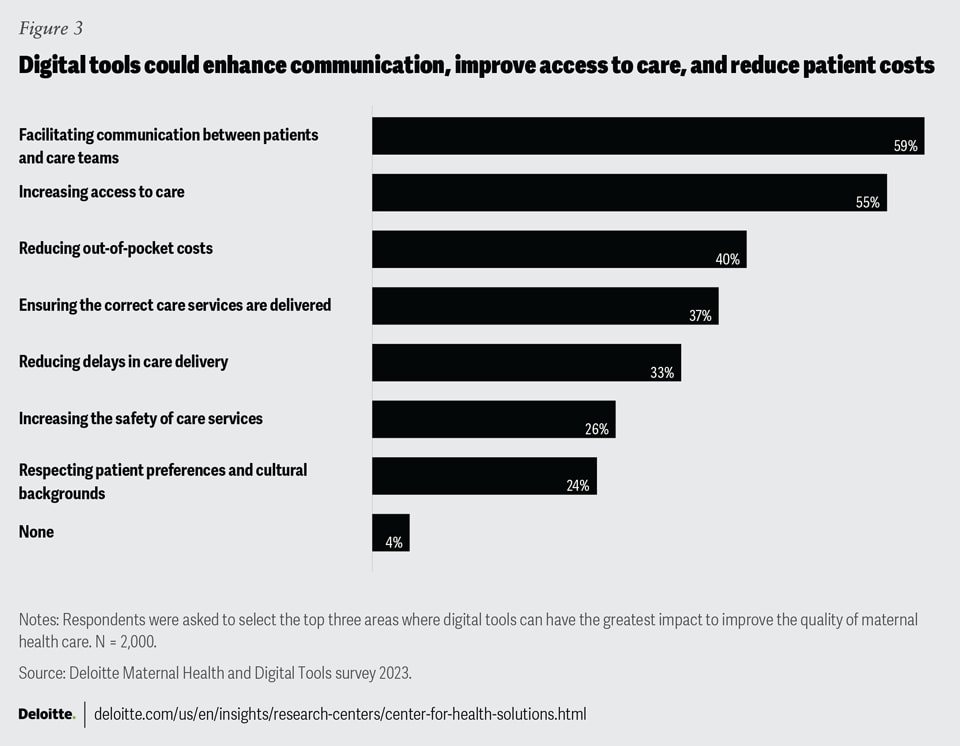
While the survey responses suggest that digital tools could significantly enhance access to maternal health services, there's broader potential for these tools. In fact, nearly 60% of respondents report that digital tools can improve communication with care teams, 55% believe they can increase access to care, and 40% think they can help reduce out-of-pocket costs (figure 3). Some interviewees also noted that digital tools can contribute to a more empowered ecosystem by reinforcing patient voices and experiences with actionable data.
Using data collected from digital tools to amplify patient voices
Digital tools can give patients more agency during interactions with their providers by supporting their concerns with trending data points—thereby empowering them at a deeper level. According to the leaders we interviewed, when patients express their concerns about pain, headaches, lack of fetal movement, or other symptoms, for example, providers don’t always know what to do with the information. Instead, when patients can share data that shows their blood pressure changed or that the fetal movement pattern wasn’t consistent during the previous few days (see “Empowering patients with data to prevent stillbirth” for more information), providers can be better equipped to act.
Empowering patients with data to prevent stillbirth
Stillbirth, the loss of a baby at or after 20 weeks of pregnancy, occurs in about one in 175 births in the United States. To put it into perspective, the stillbirth rate is about six times the number of sudden unexpected infant deaths.8 Changes in fetal movements—particularly decreases or increases in the number of movements or changes in the strength of movements—can be signs the fetus might be in distress.9 Educating and encouraging people to monitor fetal movements is a low-cost way to potentially prevent poor outcomes.10
One fetal monitoring tool is Count the Kicks, a stillbirth prevention program that could help parents track fetal movements and recognize patterns. Through an app, the organization’s website, wristbands, or paper charts, parents can count the number of movements they feel. A timer records the amount of time it takes to reach 10 movements, and parents are asked to rank the overall strength of the movements during that session. By collecting daily data, parents can determine if there have been changes in fetal movements, such as taking more (or less) time to reach 10 movements.
Founded by five mothers in Iowa who all suffered a stillbirth or infant death, Count the Kicks has helped contribute to decreasing Iowa’s overall stillbirth rate by about 32% in 10 years and during the first five years, decreasing the stillbirth rate of Black mothers in Iowa by 39%.11
The trending data collected by the app has often been referred to as a “data download for mom’s intuition.” Many mothers who have used the app have noticed that providers have taken their concerns more seriously after seeing the change in data, and then been able to act on that data.12
Making digital tools more equitable and better aligned to consumers’ needs
In analyzing the survey results, we examined different dimensions of the pregnancy experience to understand how supported the respondents felt. We looked at whether during the pregnancy journey, respondents felt their health care teams listened to their needs, believed what they were saying, integrated their preferences into their care plan, and treated them fairly and justly. Sixty-three percent to 73% of respondents reported that these aspects happened often or always during their pregnancy journey (figure 4).
However, 27% to 37% of respondents said that these aspects of care did not frequently occur on their patient journey. Those with negative pregnancy experiences were more likely to be Black or African American, and to say that digital tools were not designed to address their personal needs or align with their cultural background.
In our survey, Black (30%), mixed-race (24%), and Hispanic (23%) respondents were nearly twice as likely as White (13%) respondents to say that digital tools for maternal health need to be more culturally informed. This could mean providing the information in different languages for comprehension, showing what conditions or risk factors might look like on different skin tones,13 or accounting for cultural stigma related to certain topics like mental health.14 Cultural tailoring is important for uptake and effectiveness and is likely to continue to be important in light of persistent maternal health inequities.
We interviewed a few leaders from remote care startups who noted that depending on patient needs, they may offer services in different languages and account for cultural concordance of the care team (see “Providing culturally informed care to patients” for more information). Culturally concordant care—in which the care team or provider leverages shared cultural similarities or lived experiences, particularly for patients from marginalized backgrounds—has been found to enhance patient care experiences, improve communication between patients and providers, encourage more frequent use of recommended health care services like screenings and checkups, and decrease overall costs through more efficient care use.15
According to Deloitte research, survey respondents, particularly Black respondents, say it is important to receive care from clinicians who can understand their background.16 Interviewees, particularly those providing direct patient care either virtually or in person, noted the importance of hiring clinicians from diverse backgrounds that either share similar life experiences as patients with marginalized identities, or who can provide culturally informed care. A startup leader we interviewed noted that a virtual platform allows for more personalization and tailoring, as certain populations that may be difficult to reach in person can be helped in greater numbers online. For example, this approach could help clinicians customize care for patients with limited mobility, certain religious affiliations, or intersectional identities more efficiently and effectively.
Providing culturally informed care to patients
Mohamed Kamara lost his sister to hemorrhage and his aunt to preeclampsia.17 These experiences are the motivation for InovCares, a maternal health app Kamara founded to connect women from diverse cultural backgrounds with culturally aligned providers both virtually and in person. The app was built to address the challenges that pregnant patients from diverse cultural backgrounds typically face, including long wait times, high costs, and reduced access to prescriptions, as well as provider-specific challenges, including administrative and reimbursement issues.18 Every clinician who works with InovCares completes an intensive culturally informed training, including a focus on health equity, implicit bias, and active listening. A range of providers, from obstetricians to specialists, doulas, nutritionists, and mental health providers, are available for users through the app.19
In addition, InovCares provides remote patient monitoring (hypertension, diabetes, portable ultrasound), health assessments, health tracking, prescription delivery, community support, and education. From drivers of health to access to the internet, InovCares works to meet the needs of its users whether at community health centers, private practices, or through their health plan. It has been able to catch prenatal and postpartum conditions earlier, thus providing treatment earlier, and has been a resource for patients.20
Digital maternal health offerings should be designed for equity. Equity-centered design is a process that purposefully and continuously incorporates the real-life experiences of the end users. In this process, end users are valued as co-designers and their input is considered important throughout the entire design journey.21 Over 80% of our survey respondents indicated that people with relevant lived experience should be involved before a digital resource for maternal health is created, while it’s being developed, and after it’s launched. Furthermore, respondents also said that they would be willing to participate in each of these stages, with 87% of respondents willing to inform before development, 91% during development, and 92% after a tool is in market. These findings were consistent across racial groups.
Equity-centered design isn’t merely about ticking boxes on a static checklist. Instead, it should be an ongoing process that emphasizes active involvement and inclusion. When designing a tool or offering to address a specific issue, it is generally beneficial to bring in the experiences of those most impacted. For example, if the goal of a resource is to improve patient education on preeclampsia, then those at greatest risk of preeclampsia and with lived experience relative to the issues should inform the process.
Certain tools are specifically designed to prioritize and amplify community voices and involvement (see “Amplifying community voices to promote transparency and accountability” for more information). By bringing in community voices, digital tools can connect parents and families with similar or different experiences to provide helpful insight and support to navigate the maternal health journey. Community perspectives can also offer greater transparency into care systems, not only helping families, but also advancing accountability and improvements for organizations and hospitals across the health system.
Amplifying community voices to promote transparency and accountability
Kimberly Seals Allers created and founded Irth, a platform championing “birth without the B of bias,” inspired by her personal birthing experience.22 The platform serves as a community-driven review hub, enabling users to publicly share their experiences with OB-GYNs and pediatricians. The platform helps address the need for transparency in health care, given the high maternal mortality rates overall and for Black women. Leveraging technology, Irth transforms qualitative narratives into quantitative data, helping to bridge information gaps, foster transparency, and support a community-driven movement toward informed decision-making by health systems, plans, and physicians.23
Irth's impact includes not only individual stories, but also actively raising awareness about experiences and disparities in health care and empowering users to make informed choices. Irth's reviews are turned into robust qualitative data to work directly with hospitals, payers, and providers to provide more respectful and equitable care. This helps to advance accountability in the health system with publicly shared ratings and reviews, and a community-centered hospital improvement process. By providing a transparent space for dialogue, the platform intends to contribute to positive change in maternal health care by establishing community partnerships and advocating for health system reform and a more patient-centric health care ecosystem.
Digital tools can be difficult for people to access and use
Survey participants expressed a strong need for consumer-friendly and accessible digital resources. In particular, the respondents highlighted the need for better access, improved integration and interoperability, and less information overload.
- Increase access by reducing costs: Nearly half of the respondents (49%) noted reducing the cost of tools and related digital services as a key improvement going forward. Access to tools is merely the starting point. The economic impact of poor maternal health is already substantial, and economic challenges to solutions may also compound the problem.
- Improve integration and interoperability: Nearly a quarter of the survey respondents noted the lack of interoperability as a challenge when using digital tools. Interoperable tools allow multiple users to access data from different systems and use that data to coordinate care.24 Across all subgroups, over half of respondents indicated a need to develop a unified platform for maternal health information in the future. Structural factors like integration (within an organization) and interoperability (between organizations) can be important to translate data in a timely manner to deliver better informed care.
- Limit information overload: Across all subgroups, nearly 30% of the respondents stated that they had difficulty deciding which tool to use because there were so many options, and that too much information was causing stress. Relatedly, 44% of respondents highlighted a need to make it easier to understand how to use tools. Digital offerings should consider the information load and its impact on users’ ability to use tools effectively and make decisions for their health. While digital tools can bridge gaps in access and resolve specific needs, they should not compound maternal health burdens.
The intersection of trust, privacy, and digital tools
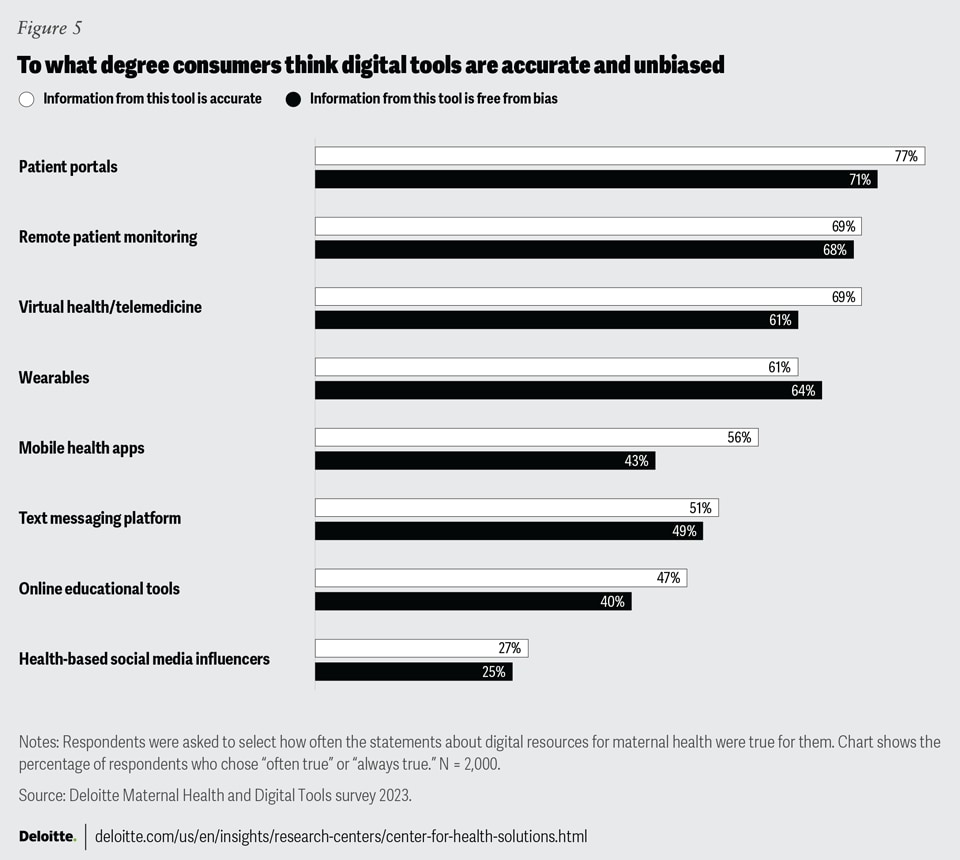
When respondents were asked about the degree to which they felt a certain tool was accurate or unbiased, patient portals ranked the highest at more than 70% (figure 5). This finding presents a potential opportunity to design and deploy resources around the patient portal as a platform that may facilitate trust more broadly, perhaps even in other types of tools.
Survey results also show that wearables have room for improvement in increasing accuracy, and mobile health apps have room for improvement on accuracy and bias. Text messaging platforms need even greater improvements on both an accuracy and bias front. Interestingly, the leaders we interviewed indicated many technology startups have found that text messages are an easy-to-use and inexpensive way to reach more patient populations, thus improving equity of access to technology.
Beyond trust in the accuracy of the information provided by the tool, there appear to be concerns about the usage of the data that feeds into the tool. Deloitte research shows that the trust gap is higher in women, and technology companies should help overcome this gap by giving consumers more control over their data and creating transparency around how the data is being used.25
Overcoming governance challenges and leveraging regulatory momentum
Prior Deloitte research shows that governance and organizational ownership of digital health initiatives are a challenge. Various departments from strategy, clinical, innovation, and marketing to security have a vested interest, leading to fragmentation. The leaders we interviewed noted a discrepancy in that consumer-facing tools are generally managed under marketing, while hospital-centric tools are often managed under IT, with confusing navigation between the two. Leveraging various departments and roles to account for applicable intersections is important, however, organizations should break siloes and clarify roles and shared ownership.
Beyond governance within the health system, the regulatory landscape across the health ecosystem can play an important role in generating momentum for equitable digital transformation in maternal health. Released in 2022, the White House Blueprint for Addressing the Maternal Health Crisis provides support for innovation in maternal health and increasing access to digital tools to advance maternal health equity.
Another challenge we heard from our interviewees is how the lack of reimbursement impedes the adoption of digital health options and add-on services. In our survey, 40% of respondents highlighted the need to cover digital tools and technologies under an insurance plan. Looking ahead, overcoming these challenges and leveraging supportive policies can help pave the way for a more accessible and equitable digital health landscape.
Digital tools are not a cure-all
In story after story, women with lived experiences have called attention to how their questions and concerns have been met with skepticism and disregard. From a former professional athlete detailing postpartum care concerns,26 to Black health professionals, including a pediatrician and an epidemiologist who died from postpartum complications,27 to a fatal outcome after a routine cesarean section,28 the list is long.
We conducted multivariable regression analyses of our survey data (a technique that allows us to account for more than one factor at a time) to understand the relationship between digital tools and pregnancy experiences. We accounted for digital tool use and utility, as well as personal factors like age, insurance status, education, and race. We found that Black respondents were significantly less likely to report a positive pregnancy experience, and digital tools did not account for the entire association with pregnancy experience (see “Appendix” for more information).
Despite their potential, digital tools are not a cure-all for the pervasive gaps across the maternal health ecosystem. Instead, the focus should be on how digital tools can be used alongside and to enhance other interventions, including in-person interactions. As one interviewee said, “We can’t deliver a baby through a screen.” Some startups have developed tools that help ensure consumers have in-person touch points, so that the human aspect of care is not lost. Equity- and patient-centered care across in-person delivery and interactions remains paramount, and the impact and resolution of this work should not fall on one sector or one setting.
Addressing maternal health inequities requires coordination across the ecosystem
The need to advance equitable maternal health goes beyond the traditional health care system. The economic impacts of poor maternal health extend to the workforce. Nearly 1.5 million mothers left the workforce in 2021 due to lack of maternal and child support, with Black, Hispanic, and Asian mothers hit hardest.29 Having fewer women in the workforce costs the US economy $650 billion annually, with $237 billion in lost wages alone.30 With an increasingly diverse national population and workforce,31 sectors within and outside of the health system should leverage their respective strengths to support patient-centered and equitable care, in person and remotely.
Health systems, tech developers, employers, and regulatory bodies alike can impact the design and implementation of digital tools as a supplement to better hybrid care. Providing access to digital tools or positioning the tools to increase access to care is just the starting point. Here are a few potential actions that stakeholders across the ecosystem could take to help improve maternal health:
- Define where and how equity, data, privacy, and trust intersect with product or service development and deployment.
- Tailor resources to meet specific personal and cultural health needs and make them easier to use.
- Diversify the data that informs the development of resources to not only include patient experiences, but also pair clinical information with the social, economic, and environmental drivers of health relevant to the broader health ecosystem.
- Collaborate with other sectors to address maternal health needs and meet patients and families where they are.
- Engage equitably by listening to those most impacted and incorporating voices into the development of product and services. Also, provide a clear feedback loop for communities, families, and patients to have a meaningful voice in the process.32
As we look at what could be possible in the future of maternal health, it's clear that the traditional approach should evolve. The task at hand is not just about elevating the standard of care, but also crafting strategies that are as unique as the patients they serve. Stakeholders both within and outside the health system can champion equity and empowerment. And digital tools should be developed such that they are effective, bias-free, and easy-to-use. Such a transformative shift in the maternal health paradigm can contribute to a healthier, brighter future for all.
Appendix: Study methodology, respondent profiles, and data analysis
1. Study methodology
The Deloitte Center for Health Solutions conducted a survey in the United States in July and August 2023 of 2,000 people ages 18 to 54 who were pregnant in the previous two years. The sample included a nationally representative group of Asian, Black, Hispanic, White and multiracial respondents. We oversampled those who identify as Black or Hispanic, as well as individuals with an annual income lower than US$50,000. Age, race, and ethnicity were weighted to be representative of 2022 Centers for Disease Control and Prevention natality vital statistics data.33 Region, income, and education were weighted to be representative of all women ages 18 to 54 in the US census.34 We asked about their use of digital tools, including patient portals, mobile health apps, online education tools, wearables, telemedicine and virtual care, text messaging platforms, remote patient monitoring devices, and health-based social media influencers. To supplement the survey findings, we interviewed 20 executives from maternal health–focused organizations in the United States comprising academic medical centers, digital health technology startups, community-based organizations, health systems, clinics, and professional and patient advocacy groups.
We also led a focus group discussion in May 2023 with 10 hospital and health information executives associated with the College of Healthcare Information Management Executives. We recognize that there is no one definition of what a family looks like and who is on the maternal health journey. In this paper, we refer to women, mothers, families, patients, pregnant people, people with relevant lived experience, and consumers broadly to reflect the various ways our society experiences maternal health.
2. Deloitte Center for Health Solution’s Maternal Health and Digital Tools Survey 2023 respondent profiles
3. Data Analysis
- All reported survey findings are based on descriptive statistical analyses of comparisons among groups. We report statistically significant findings, with significance tested at a p-value less than 0.5.
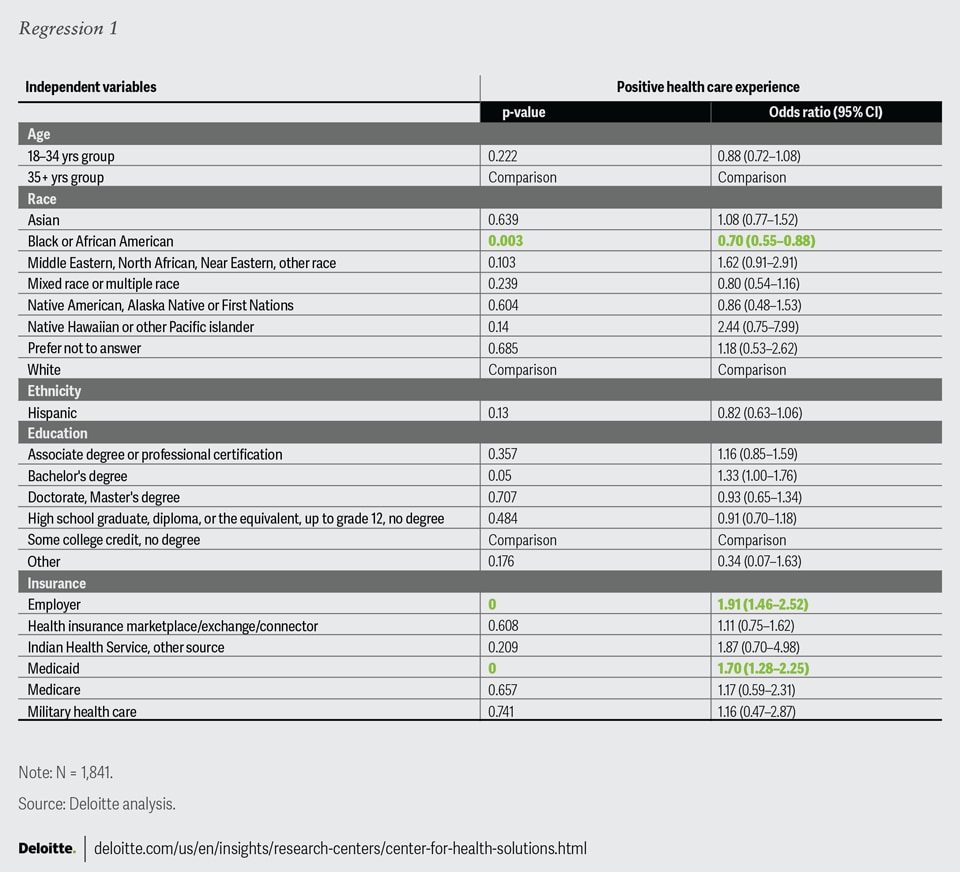
- Regression analyses: To better understand factors related to maternal health experiences, we used multivariable regression analyses on 1,841 survey responses, comprising those who used digital tools during their pregnancy experience. The outcome or dependent variable of interest is a positive pregnancy experience. This is a composite binary outcome based on responses to whether in their prior pregnancy experience, respondents were always or often listened to, believed, had their preferences integrated into the care plan, and treated fairly and justly.
- In the first regression, we examined the influence of sociodemographic measures (age, race, ethnicity, education, and insurance source). Age, race, and education are categorical variables (see “Appendix” regression table for categories). Ethnicity is a binary response, given its potential overlap with race. Insurance options are also treated as separate binary options, as respondents could have more than one insurance source. Findings show a positive relationship between employer-sponsored health insurance, Medicaid insurance, and a positive pregnancy experience, but a negative relationship for Black or African American respondents.
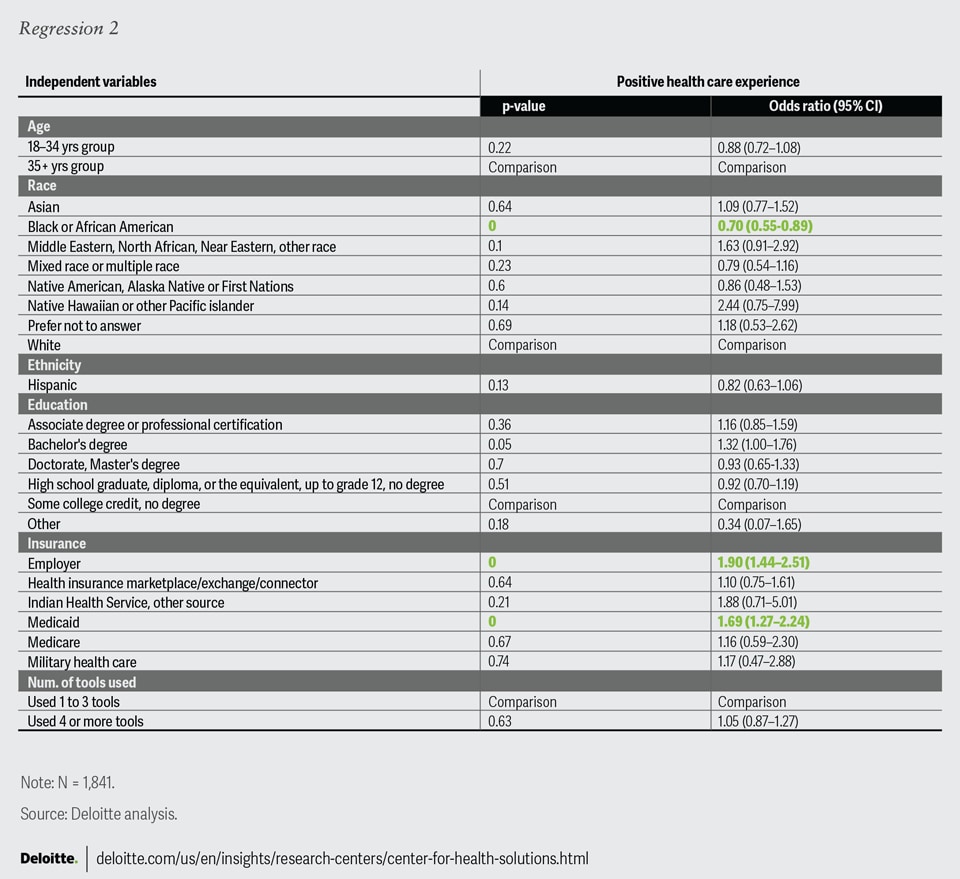
- In the second regression, we controlled for the same sociodemographic measures and examined whether the number of tools used (binary variable of low, up to 3, vs. high, 4 or more) was associated with indicating a positive pregnancy experience. The number of digital tools was not associated with the outcome.
- In the third regression, we controlled for the same sociodemographic measures and examined whether the types of tools used (binary variables for each tool) were associated with indicating a positive pregnancy experience. We observed a positive association for those using patient portals, but a negative association for those using social media influencers.
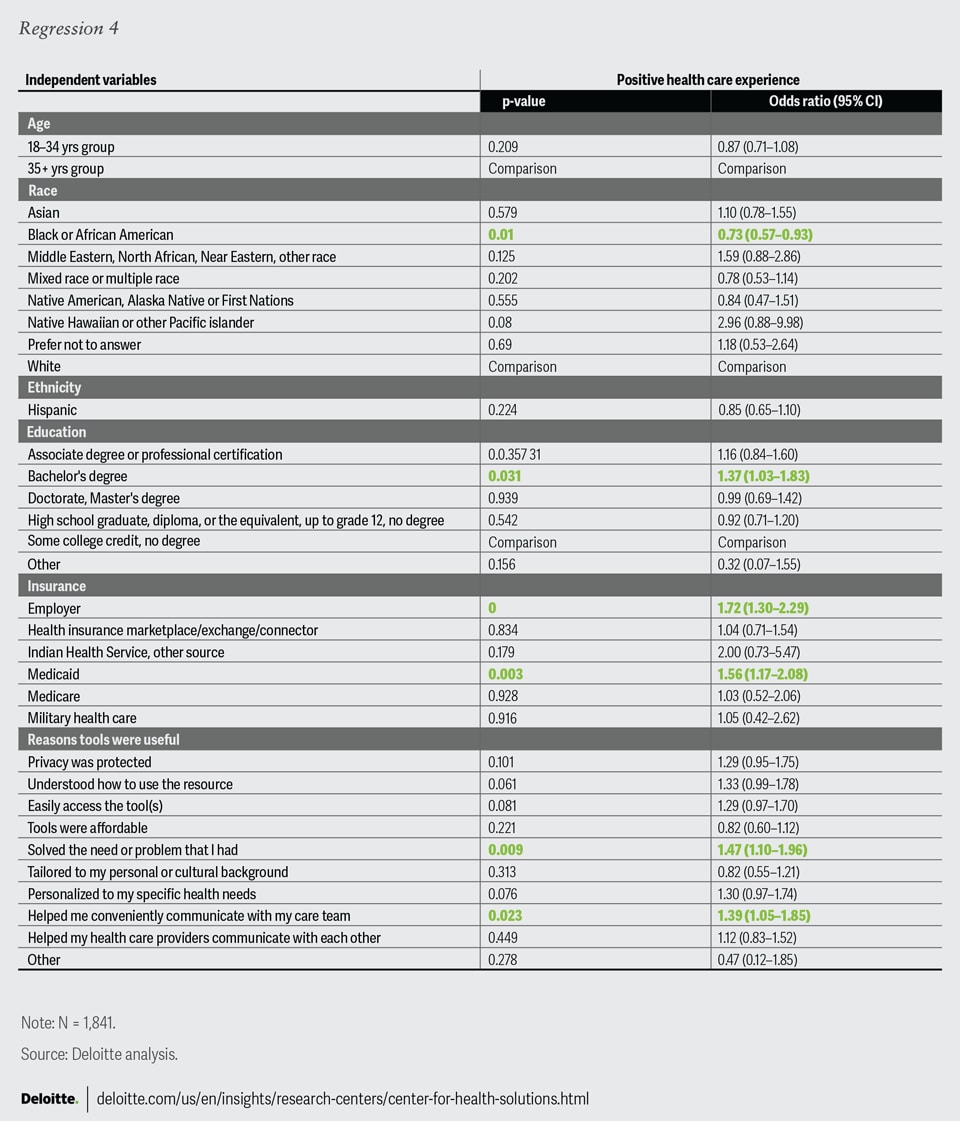
- In the fourth regression, we controlled for the same sociodemographic measures and examined whether the utility of the tool was associated with indicating a positive pregnancy experience. Utility due to convenient communication with the care team and solving specific problems or needs had a positive association with the outcome.
- The significant insurance and race relationships we observed remained stable across all regressions. Based on the negative statistical association for Black respondents, we also explored statistical interactions for Black respondents, insurance access, and the significant tool measures. However, these did not significantly change the primary finding that access to care and digital tools does not completely account for the quality of the pregnancy experience for Black respondents.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}