













{kind=link}
{kind=link}
Enhancing clinical trial diversity has been saved
Deloitte authors include Christine Chang, Jessica Overman, Greg Reh, Wendy Sanhai, Sonal Shah, and Alexandria Younossi.
PhRMA authors include Maria Apostolaros, Courtney Christian, Rebecca Marklund, Jim Mayne, Allison Morgan, Rich Moscicki, and Mary Nwokedi.
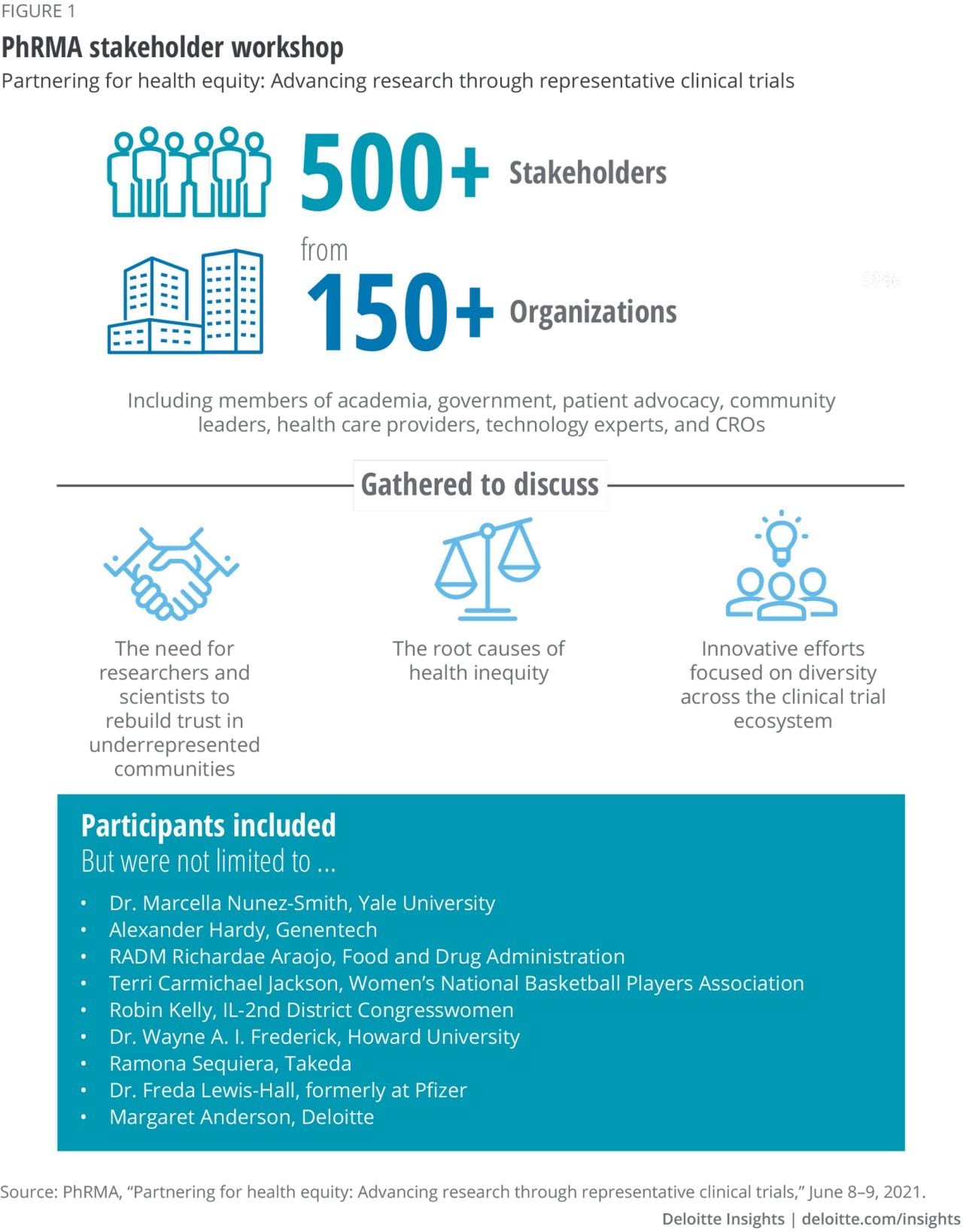
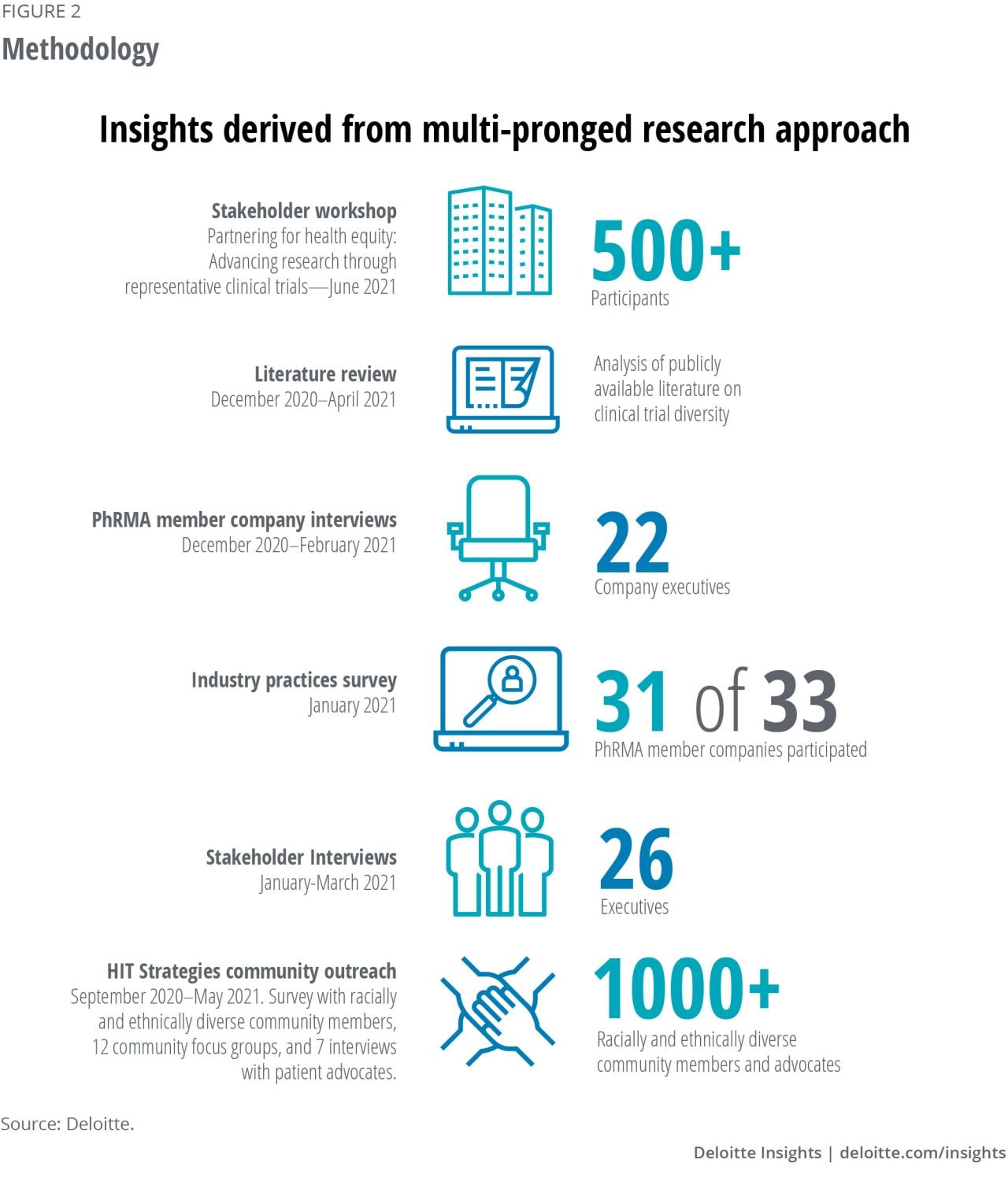
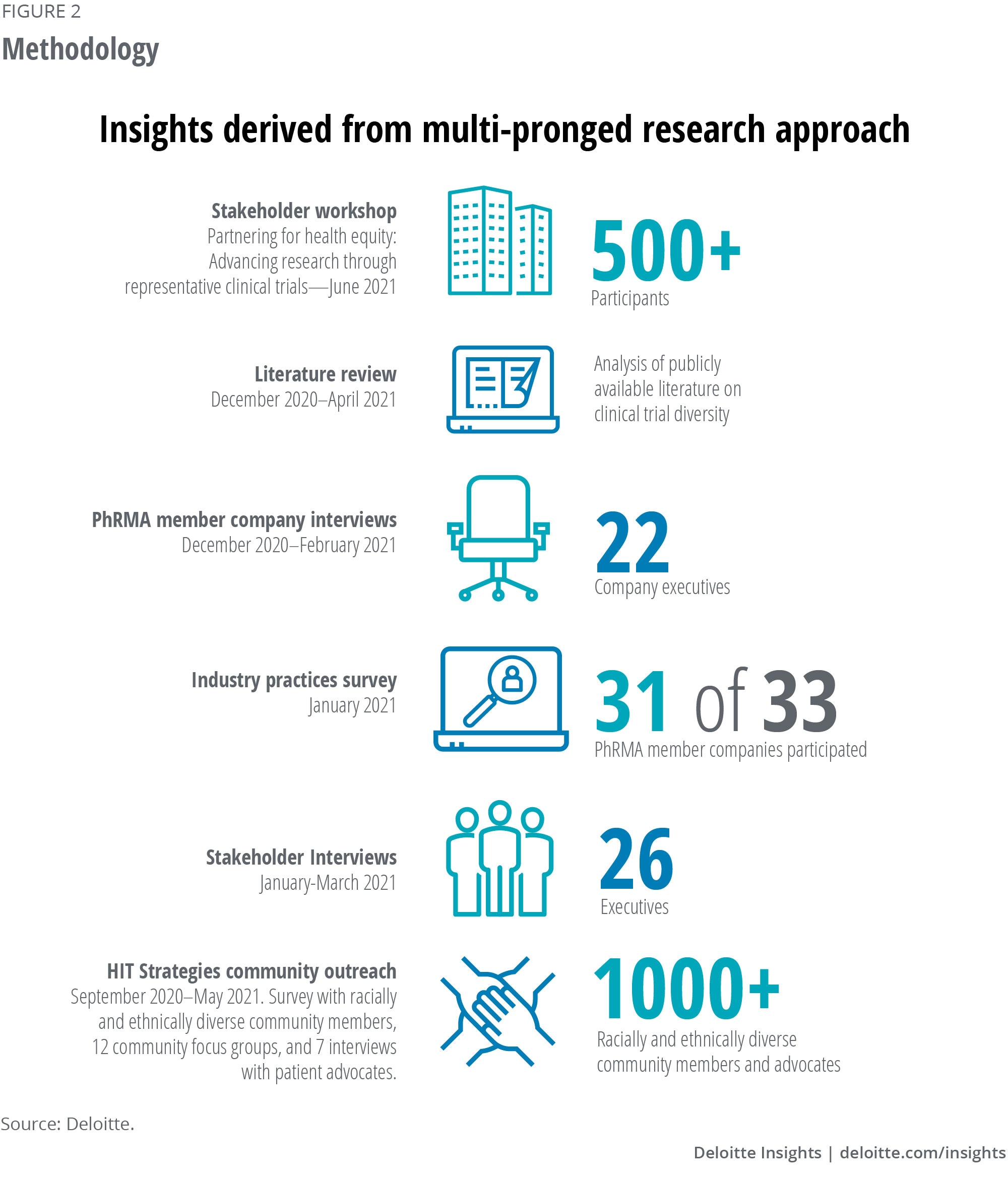
The authors would first like to thank Pharmaceutical Research and Manufacturers of America (PhRMA) member companies who participated in interviews, the survey, and the workshop. The authors would also like to thank the many industry stakeholders who participated in interviews and the workshop. This report would not be possible without their contributions.
The authors would like to especially thank Dr. Freda Lewis-Hall for her guidance and insights throughout this research.
This year-long collaboration required significant effort to execute research, analyze data, engage stakeholders, develop insights, and write, edit, and produce the report. The authors would like to thank Elizabeth Baca, Zion Bereket, Anna Bianculli, Andrew Bolt, Tina Bressert, Ashley Daniels, Linda DaSilva, Steve Davis, Mike DeLone, Laura DeSimio, Asif Dhar, Kevin Dondarski, Kulleni Gebreyes, Kelly Goldberg, Kevin Harris, Blythe Hurley, Neil Lesser, Nile Marshall, Aline Mnayan, Ramani Moses, Bushra Naaz, Sastish Kumar Vnkata Nelanthula, Heather Nelson, Angie Paik, Matt Plitch, Amanda Pratter, David Rabinowitz, Negina Rood, Sarah Shier, Sanjay Mallik Vadrevu, Navya Vantakala, Tim Vaske, and Lucy Vereshchagina.
Cover image by: Alexis Werbeck