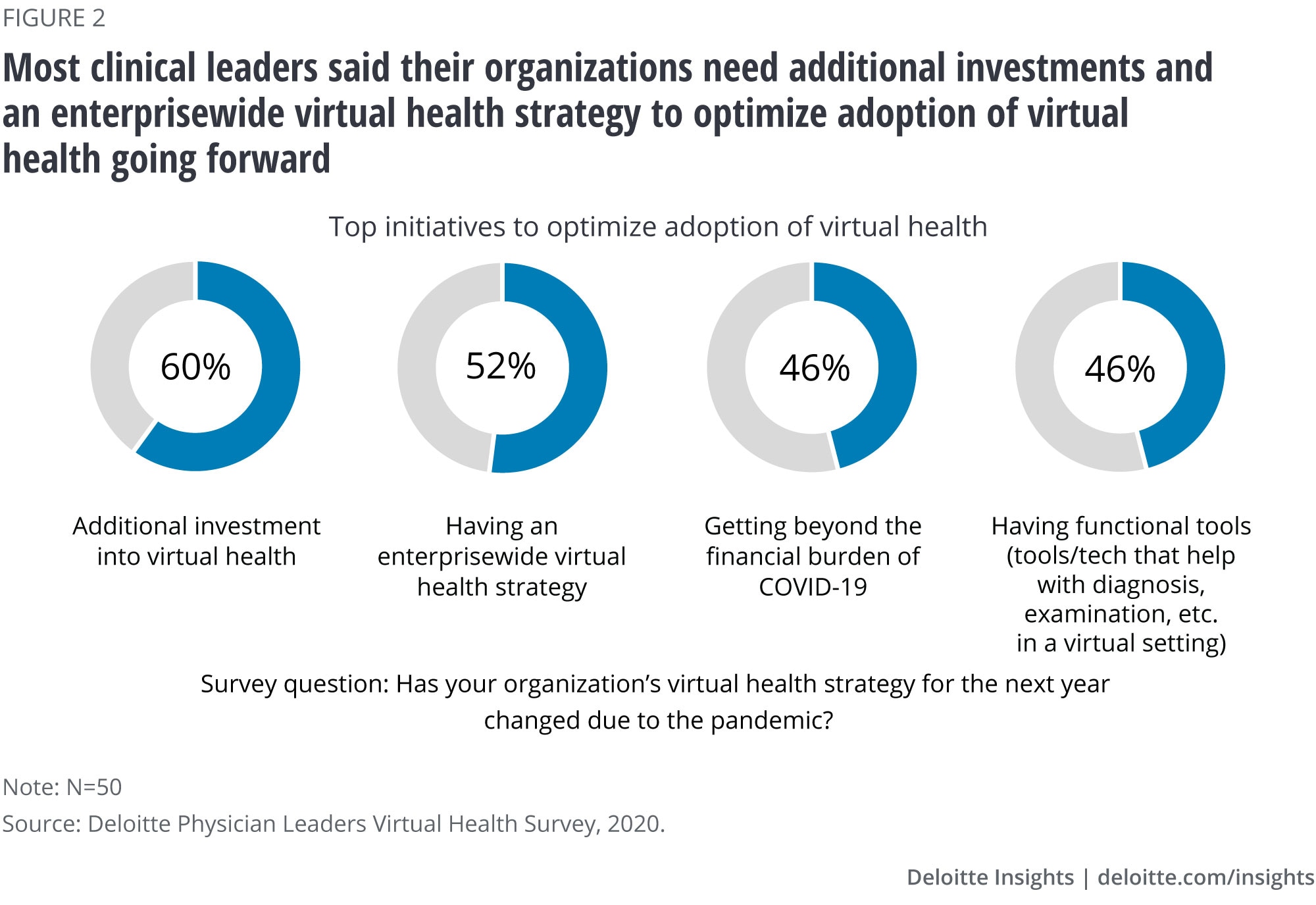
Our research participants agreed that, as health systems refine strategies and adopt new models, they should be mindful to avoid some of the mistakes that were made during the early years of the electronic medical record. Long before the pandemic, physicians were experiencing frustration and burnout from screen time and administrative fatigue.6 A recent study shows physicians were satisfied with virtual visits when they had input into how they were used, had administrative help, adequate payment, and access to reliable and easy-to-use technology.7 We expect to see increased investments in remote monitoring and patient wearables in the coming years. This will likely be driven by growing investments in digital health,8 and demand from clinical leaders. Half of the clinical leaders we surveyed said they wanted more functional tools and technology to optimize virtual health (figure 2). Health system leaders should think through how to seamlessly integrate those tools and platforms so that they enhance clinical care rather than add work for clinicians.
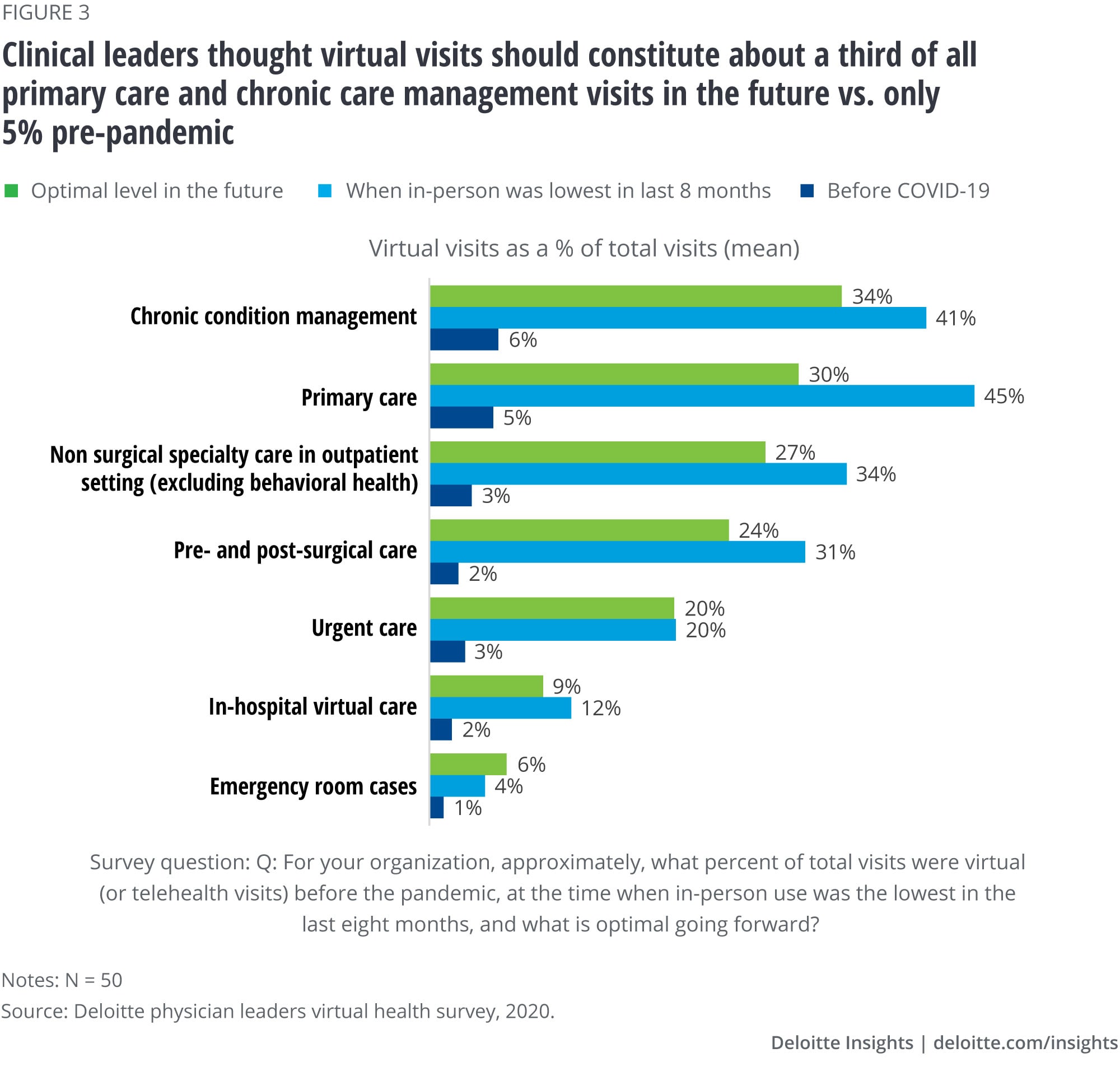
Across care settings, clinical leaders describe the optimal level of virtual visits as being close to the peak they witnessed during the pandemic
During our roundtable discussion, physician executives said they were interested in determining the optimal level of virtual visits for the future. Clinical leaders we surveyed indicated that the optimal level of visits over the next one to three years could be similar to the peak volume they saw during the pandemic.
When face-to-face visits reached their lowest point during the pandemic, virtual visits for primary care and for chronic condition management peaked at 45% and 41%, respectively (figure 3). Virtual visits for nonsurgical specialty care in outpatient settings (excluding behavioral health) peaked at 34%. Clinical leaders agreed that the optimal level of virtual chronic-condition management and primary care will be about one-third of overall visits. Prepandemic levels of virtual visits for those areas of care were around 5%. This willingness to continue virtual visits at levels that are close to the peak seen during lockdowns could be good news for the continued growth of virtual health.
We asked clinical leaders which areas of hospital stay they expect would be most impacted by the acceleration of virtual health. A majority of them said that there could be a significant increase in virtual technology for prestay scheduling and reminders, postdischarge chronic-care check-ins, patient monitoring, and follow-ups in the coming months and years.
We also asked which specialties would likely see the largest uptake in virtual visits over the next one to three years. Primary care topped the list, followed by behavioral health, dermatology, and internal medicine.


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}