
Advancing health equity through community-based ecosystems
Stronger partnerships can help health systems address drivers of health and create a world in which everyone thrives.
Executive summary
Today’s health systems understand the importance of creating a world in which everyone thrives, regardless of race, ethnicity, gender, sexual orientation, disability, or age. To create a healthier society that allows all people to live to their fullest potential, health systems should consider addressing the root causes of health disparities in every community. By establishing community-based ecosystems—or strengthening the ones they’ve already formed—at the local, state, and national levels, health systems could elevate community health outcomes and directly change people’s lives.
Many health systems are working to create a healthier society for all through their long-standing partnerships with community-based organizations (CBOs), government agencies, financial institutions, locally owned businesses, philanthropic foundations, and more. By focusing on nonmedical drivers of health (DOH), also known as the social determinants of health, these partnerships are improving access to education, food, housing, and employment. This can result in a better quality of life, more preventive care services, fewer emergency department visits, and lower overall health care costs for communities.1
The Deloitte Center for Health Solutions conducted a study to understand how health care systems improve health equity by strengthening existing ecosystems and increasing connections, tools, and shared goals among the partners. To gather these insights, we interviewed 15 C-suite–level experts in areas such as health equity, diversity, equity, and inclusion from health systems, CBOs, departments of health, foundations, and technology companies and conducted an extensive literature review.
These ecosystem models have different names: public-private partnerships, collective impact, stewardship, or aligned action. Regardless of the model, keys to successful ecosystems often include:
- Establishing relationships with the right partners in the community and ensuring community voices are heard,
- Creating a governance model and developing shared goals,
- Leveraging new technology platforms when possible, and
- Using existing key performance indicators (KPI) to understand progress.
Every ecosystem will be unique to its geographic area and its participants. Health systems and their partners should consider new ways to learn more from each other and be willing to include, listen to, and truly engage people who live in the community and learn from their lived experience, for they are the ones who know what the community needs. While sustaining ecosystems isn’t without challenges, partnerships that evolve into ecosystems can have a greater impact on the drivers of health and the health of their communities.
While sustaining ecosystems isn’t without challenges, partnerships that evolve into ecosystems can have a greater impact on the drivers of health and the health of their communities.
Focusing on drivers of health to advance health equity
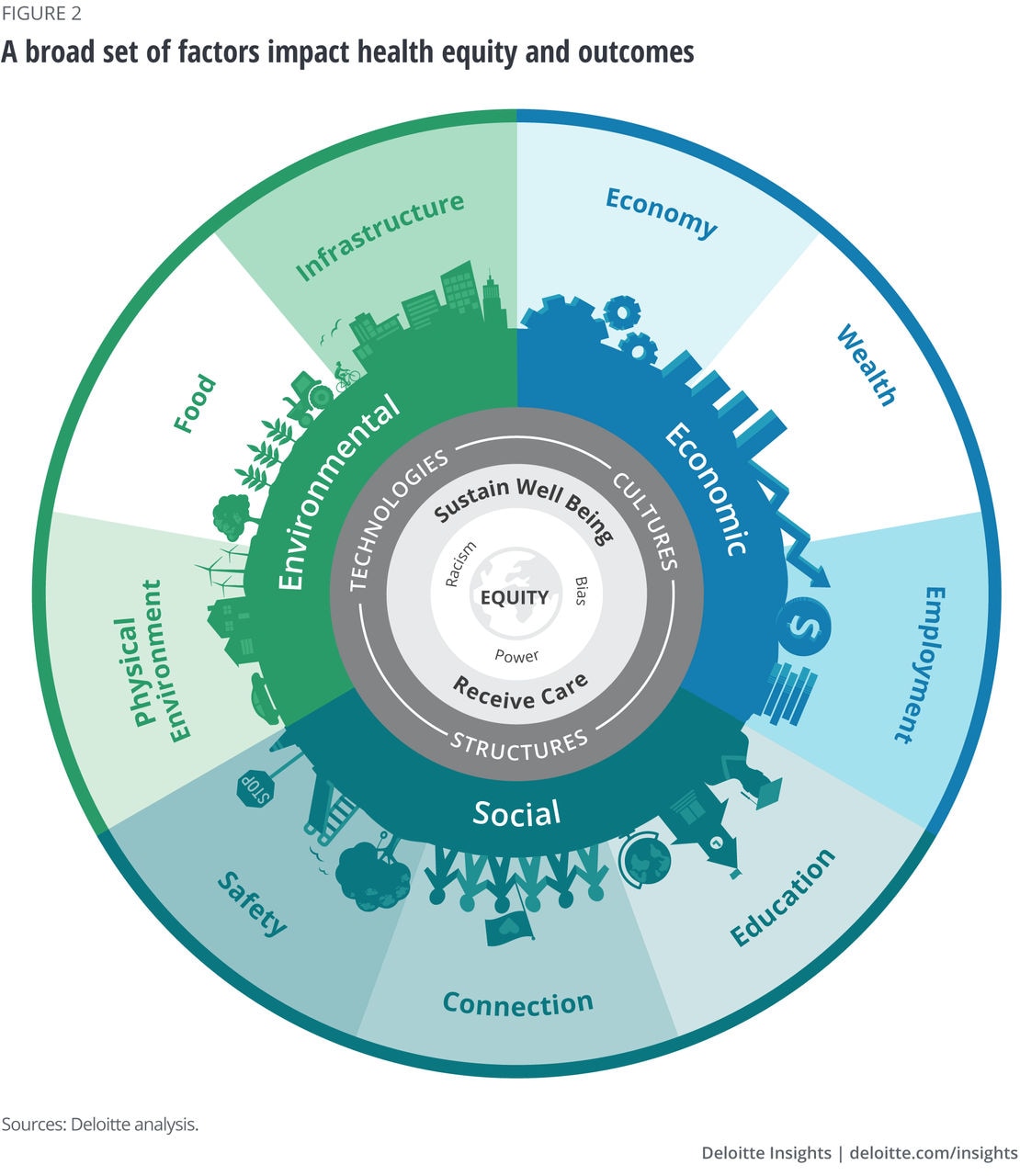
The global COVID-19 pandemic and social injustices like the death of George Floyd have called national attention to long-standing health inequities in the United States. These events and others have prompted many health systems to acknowledge the problem, double their efforts to address inequities, and work toward decreasing disparities. Health care organizations can activate health equity through multiple dimensions to accelerate progress in addressing systemic biases that lead to disparities (figure 1). As such, this paper focuses on investing in communities and amplifying efforts through ecosystems that target the drivers of health (figure 2).

Deloitte’s recent research on addressing the drivers of health highlights that one way to advance health equity is by focusing on the social, economic, and environmental needs of all community members. These factors have been found to have a greater impact on health outcomes than the care provided by clinicians (figure 2).2 According to Deloitte’s findings, 90% of health plan leaders and 74% of health system leaders said that improving health outcomes is a top goal of their organization’s DOH strategy.3 However, more than two-thirds of the surveyed respondents felt that they aren’t leveraging partnerships with CBOs enough, and more ecosystem partners are needed to bolster DOH.
Similarly, Deloitte's research on rebuilding trust in health care revealed that patient groups that have been historically marginalized and underserved want their local hospitals to partner with community organizations to help rebuild that trust. Working with CBOs, such as places of worship and barber shops, health care organizations can begin to rebuild patient trust.
Community health needs assessments (CHNAs) give health systems a community-level view of the drivers that impact their patients. CHNAs can be used as a tool to diagnose health issues in the community and as a framework to monitor and evaluate if changes have been effective. Community-based ecosystems offer an opportunity to rethink the CHNA process and work toward better health outcomes, while helping health systems build stronger relationships and make concrete investments to address community needs.
Community-based ecosystems—smart health communities are one example—already exist in many communities, but how engaged they are in addressing DOH varies. Supporting the efforts of existing players and adding critical partners can enable community-based ecosystems to build on their current work and improve community health outcomes for more stakeholders.
“If people are really wanting to address health equity, that requires changing structures and systems, and no single organization can do that on their own. An ecosystem approach is what we need to change the systems and the structures that are holding the problem in place.”—Executive director of a nonprofit organization
We define a community-based ecosystem approach as:
- Bringing together multiple players to create, scale, and align impact in ways that are beyond the ability of a single organization
- Addressing complex issues through a diversity of experience and expertise, and a collective ability to learn, adapt, and innovate
- Having a shared vision and understanding of the problem, and explicit resources to coordinate, monitor progress, and adapt
To understand how leading health systems are strengthening their ecosystems to better address health equity, the Deloitte Center for Health Solutions conducted 15 interviews with individuals at organizations that participate in ecosystems. Interviewees included CEOs, COOs, executive directors, chief people and culture officers, chief health equity officers, and chief diversity and inclusion officers at health care organizations, CBOs, health departments, foundations, and technology companies. From these interviews, we gathered some leading practices for health systems that are looking to strengthen their existing partnerships and move toward an ecosystem approach to advance health equity in their communities.
Establish the right partnerships and ensure the community’s voice is heard
We learned from our research that finding the right health ecosystem partners is an important key to success. But how the partnerships are established matters, too. It’s typically easier to establish relationships with a few key partners, create a shared vision, and then grow into a larger coalition than it is to bring together multiple entities at once.
Health systems should consider partnering with nontraditional partners such as pop-up shops, small grant givers, and businesses that provide innovative financing options. At least one of the partners should be a local individual or organization that has credibility, lived experience, and history in the community. Additionally, the ecosystems should represent a range of diverse communities, including racial and ethnic diversity, people with disabilities, populations in rural or geographically isolated areas, older adults, low-income populations, and LGBTQ+ individuals.4 The key is to provide these community members with opportunities to voice their concerns and be an active part of the initiatives. These individuals need more than a seat at the table; they should have the power to drive the agenda, which requires a change in the way most health systems have worked with the community in the past. Having all groups represented can be critical to influence and affect desired change because they each will have important perspectives on what problems are most pressing and what interventions are most beneficial for improving their lives.5
“If you want the project to go forward, you’ve got to recruit somebody that has more history and credibility in the community.”
— President and CEO of a community development organization
Approaching and engaging community members will require thought and cultural humility as well as a willingness to listen, learn, and change the decision-making process. Traditional players should leverage the vast knowledge and depth of experience offered by community members to improve the effectiveness of health programs. The interviewees noted that many of these community-driven, grassroots efforts continue to follow a traditional top-down approach. As a result, they often don’t harness the power of or recognize the value that the community brings to the collaboration.
The interviewees agreed that health systems have an opportunity to become more actively engaged in community-based ecosystems. Because health systems are important employers and drivers of economic activity in their communities, they’re uniquely positioned to proactively build partnerships and participate in community engagements. Building community-based ecosystems can benefit health systems in the following ways:
- Improve health outcomes. Health systems are driven by missions to deliver the best and safest care they can to communities. According to our interviewees, when health systems participate in community-based ecosystems, they can drive health outcomes that are difficult to achieve on their own. The outcomes include decreasing emergency department visits, improving preventive health, increasing quality of life, and reducing overall costs 6—all important metrics for accountable care organizations (ACOs).
- Build consumer trust. Health systems that are actively involved in community engagements can build trust and improve community health. Based on focus group research, Deloitte found that consumers may be more willing to get care and preventive services through trusted CBOs such as community centers, barbershops, or religious organizations. By partnering with these CBOs, health systems can be better able to provide culturally appropriate health messaging and a relatable forum, which often results in better health outcomes.7
- Gather more patient data. Shared data between ecosystem partners allows health systems to better understand their patients, which can aid in care, improve follow up approaches, and result in better outcomes. Broader data initiatives, such as Data Across Sectors for Health (DASH), have assisted communities in building capacity for data-sharing to improve health equity.8
Conversely, health systems can bring many skills to the ecosystem such as operational expertise, bandwidth to make community investments through grants and other mechanisms, resources to analyze data, and political will to make local policy changes. Health insurers also can play a vital role in ecosystems by embedding DOH more fully into ACOs, value-based care, and other agreements, changing reimbursement policies to include DOH-related services, collaborating with providers, and coordinating activity within an ecosystem.
Just as every ecosystem is unique, health care organizations can participate in ecosystems in different ways. One option is to co-lead an ecosystem with a CBOs. This approach requires a larger investment of both people and resources. Alternatively, a health care organization could choose to be a participant in an ecosystem, focusing on providing expertise when it’s most helpful. Either way, the ecosystem approach requires organizational change because it’s typically more effective when the whole organization is involved, understands the benefits, and can connect the effort to individual patient interactions.
“Community development efforts cannot be driven by just one sector or one organization. It takes multiple partners to work together.”
— CEO of a technology company
Create a governance model and develop shared goals
There’s a wide range of governance models for ecosystems and settling on the right one often depends on the needs of the individuals and organizations involved and the amount of funding available. Public-private partnership and aligned action are two types of models, though the collective impact model is the most well-known in the social sector (see sidebar, “What is the collective impact model?” for more information). In general, the amount of funding that’s available determines how formal the governance approach is. Some community-based ecosystems, such as the Magnolia Community Initiative, follow a less formal structure (see sidebar, “Magnolia Community Initiative,” for more information). Participation is by self-selection and based on how much time and resources organizations can commit to the shared goal. Through monthly network meetings, working groups, and improvement projects, the network partners collaborate, brainstorm new ideas, and turn them into reality.
Other partnerships, such as the Lachman Community Development initiative, are developed almost purely based on a single individual’s ability to bring people together. The initiative has partnered with faith-based institutions on food insecurity by developing community gardens, improving food distribution and access, and deploying nutrition education and counseling programs.9 Collaborating with individual partners and then bringing them together to work toward a common goal has been key to this type of approach.
“Participating organizations should contribute with “intentionality” to create a social connectedness and strengthen the community as a whole.” — Director of a community initiative
Other initiatives, such as MedLink, follow a more formal arrangement by establishing an executive committee and governance policies and procedures (see sidebar, “MedLink,” for more information). For example, they might set monthly meeting agendas and hold meet-and-greet meetings with partners twice a year for cross-pollination opportunities. Other initiatives have contracts in place between entities and/or grant funding for specific pieces of the collaboration. The collective impact model, when followed precisely, requires a separate organization with dedicated staff and a specific set of skills to serve as the backbone of the initiative to coordinate participating organizations.10
“If you want to change the system, get the system in the room.”
— Executive director of a nonprofit organization
What is the collective impact model?
The collective impact model11 brings together a diverse group of stakeholders—nonprofits, philanthropy, government, etc.—with a structured process for pursuing systems change. The collaborative approach can be applied to a city, county, neighborhood, or state, or at a broader level.
The model encourages cross-sector collaboration, engages community members, utilizes data to learn, adapt, and improve, cultivates leaders with unique skills, and builds a culture that fosters relationships, trust, and respect across participants.
Goal: Facilitate cross-sector collaboration to address complex social and environmental challenges such as health equity.
Conditions for collective success: To ensure that a collective impact initiative generates powerful results, five conditions should be fulfilled: a common agenda toward a shared vision, shared measurement for continuous improvement, mutually reinforcing activities among participants that build on each other to maximize results, continuous communications to build relationships, and backbone support organizations to drive the initiative.
A place-based approach, a specific type of collective impact model, focuses on a narrowly defined geographic area. This approach can produce meaningful change due to the hyperlocalized and complex nature of health equity issues. The ProMedica Ebeid Neighborhood Promise (ENP) is an example of a place-based initiative led by a health care system. The initiative addresses DOH such as health, stable housing, jobs and finances, education and training, and safety issues in Toledo's Uptown neighborhood. Over the past five years, ProMedica has pursued critical improvements to the quality of life by engaging neighborhood residents, stakeholders, and businesses to create effective initiatives that can be scaled.
ProMedica and several community partners who provide critical perspective and lived expertise are focused on four areas: improving health outcomes, increasing access to education, offering job training, and providing stable housing.12 ENP has achieved several measurable outcomes in the past few years. 13 More than 2,600 individuals have received financial coaching, 100 residents raised their credit score by an average of 46 points after partaking in financial coaching, and 55% of individuals who participated in the Ebeid job training program obtained employment. Additionally, US$13 million in impact investment capital was deployed for housing and small business development projects.
ProMedica knew that the seats at the table must expand beyond traditional “key stakeholders.” In addition, it was vital to enter communities as a collaborative partner, not just providers of services, resources, or dollars.
Magnolia Community Initiative
Goal: The Children’s Bureau of Southern California established the Magnolia Community Initiative (MCI) in 2008 with the goal of improving community outcomes and the well-being of vulnerable families in downtown Los Angeles. The community-based initiative focuses on enhancing the education, health, quality of nurturing care, and economic stability factors for children and youth situated in high-need, low-resource neighborhoods in the area.14
Partner organizations: MCI is a voluntary network of 70 partner organizations, including the Los Angeles County Chief Executive Office’s social services, child support, and child protection departments, the Los Angeles County Unified School District, the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), and community-based nonprofit organizations providing health care, early care, and education.
Participation and funding model: MCI follows the collective impact approach to solving social problems, which means that multiple entities are committed to a common goal. According to one of our interviewees, organizations self-select themselves for the initiative. Since this is an unfunded collaborative model, there’s no lead agency, third party, or neutral entity providing extrinsic rewards to community members or organizations for their participation. Individuals and organizations align their efforts and resources toward an agreed-upon set of design elements such as activating parents to address their child’s developmental needs and to care for their own physical, social, and emotional health needs.15
Community hub: MCI draws the community in by making its physical space a place that children and families want to visit. A farmer’s market outside its doors provides fresh, local produce at a low cost. The building walls are colorful and decorated with murals drawn by children. A nature center with a wall-to-wall fish tank provides a respite in one of the poorest neighborhoods in LA. The building also is a space for the community to use for performances, classes, a place to read, etc.
Single-user interface: Community members only need to fill out paperwork once to join a myriad of services including WIC, health care, and social services. By removing barriers to accessing programs, the community can fully leverage the services available to them.
Outcomes achieved in 2020:16
- Framework for healthy families: Eighty-seven percent of parents increased parental resilience, 82% of families reported having social connections, and 82% of parents enhanced the social and emotional competence of their children.
- Mental health services: Provided 109,863 hours of mental health therapy and counseling to 4,454 children and their families.
- Prevention programs: Provided 5,000 home visits to 650 at-risk families with young children in need of parent education and services. Also, more than 600 low-income children received developmental and health screenings and saw improvements in their school readiness skills.
The interviewees noted how important it is, particularly in place-based strategies, to bring the voices of the people who live in the community to the forefront (see sidebar, “The Two Georgias Initiative,” for more information). After all, they have the most knowledge about the problems they face and can help generate better solutions. Recent Deloitte research noted that very few health care organizations have developed strategies to address health equity that incorporate direct feedback from communities.17 Place-based efforts that are led by the community and centered on community can be successful, sustainable over time, and accepted by the community (see sidebar, “United Way Worldwide,” for more information).
“Place-based community development strategy must be authentically driven by the people affected or who might potentially benefit from whatever program or service is created.”
—Director of a nonprofit organization
The Two Georgias Initiative
Launched in 2017 by the Healthcare Georgia Foundation, The Two Georgias Initiative18 is a multiyear, place-based effort aimed at addressing the growing disparities in health and health care between the metropolitan areas and rural communities in Georgia. The goal is to support local coalitions seeking to improve health care access for residents in Georgia’s rural communities.
The Foundation gave US$1.1 million in funding to help 11 rural community health coalitions in Georgia develop and implement community health improvement plans. These initiatives allow the people most adversely impacted by health inequities to have a seat at the table and voice their opinions on addressing their health challenges. Here are a few examples of how the coalitions are working to create an impact:
- The Appling County coalition is engaging in cross-sector collaboration to improve access to high-quality education, jobs, and opportunities to lead a healthy lifestyle.
- The Clay County coalition is focusing on youth services, access to health care and healthy living, and adding new community members to its Clay County Health Partnership.
- The Haralson County coalition is building partnerships between residents, emergency personnel, and substance misuse prevention and treatment programs.
The leaders we interviewed note that rural communities face unique opportunities and challenges. Because people who live in rural communities often have more than one role in the tight-knit community, when forming an ecosystem, many of the individuals already know each other and have worked together before. But at the same, if there’s a difficult history between key individuals, it can make it hard to establish the relationships needed.
United Way Worldwide
United Way Worldwide (UWW) is a privately funded charity with more than 1,100 local United Ways working across 40+ countries to build stronger, more resilient, and more equitable communities.19 In its focus areas of education, financial stability, and health, United Way uses collective impact and place-based strategies to address community needs in local communities. For these efforts, UWW leverages its array of funding resources and vast network of relationships with CBOs, local government agencies, school systems, volunteer organizations, health care provider organizations, and more.
“There is power in numbers. There is so much good work going on in communities, but gaps in access and opportunities do exist. When you’ve identified your focus, chances are that someone is probably already doing work in that area. Identifying those organizations and relationship building are key. Use the resources that already exist in your community and build upon that for collective impact.”
—Director of health, United Way Worldwide.
Leverage new technology platforms
Technology vendors are building platforms to facilitate connections between partners, improve coordination, and build a network of CBOs to address drivers of health. Although these platforms are relatively new, there’s an opportunity to continue developing them as a key component of an effective ecosystem for improving health outcomes.
A platform should be designed to work seamlessly when an individual needs assistance. For example, a health system can log into the technology platform to quickly identify a partner organization with the capacity to provide the needed service. At the same time, the provider can check the individual’s eligibility and send a referral. Later, they can see if the patient received the referred service while securely sharing any relevant information with the community organization (see sidebar, “MedLink,” for more information). Additionally, the patient is able to access any appointment-related information they need via the same platform.
“By being agnostic and neutral in this space as a platform company, we can facilitate true connections across all industries.”
— COO of a technology company
However, our interviewees noted a few technology-related challenges. For example, a permission-based privacy model—in which consumers can safely and securely self-navigate the available services, view their personalized recommendations, and share information with their preferred physician or health care organization—hasn’t been fully developed on these platforms. Better defined data standards and interoperability requirements could help ecosystem participants track outcomes and share information. And recognizing that patients have different access to and literacy of digital tools will be important to prevent widening the digital gap.20
MedLink
MedLink of Mecklenburg County, N.C., is a coalition of safety-net service providers, focused on providing equitable access to care through education, communication, and collaboration.21 MedLink advocates for access to care through their mission of amplifying the voice of the underserved in the community to ensure all have access to effective, efficient and coordinated care. Service providers are defined as governmental and nongovernmental organizations which support community health efforts through direct patient care, patient support, education, and advocacy. MedLink initially went live with a pilot cohort of seven community partner organizations, but the initiative has grown to include 19 partners including shelters, legal advocates, and community clinics. Headquartered in Charlotte, NC, MedAssist is part of the coalition’s executive committee.
Governance structure. The executive committee and voting members of the coalition are responsible for creating governance policies and procedures and setting monthly meeting agendas. The decision-making process during meetings takes place using a simple majority of voting members. Voting member agencies are required to pay dues annually, to ensure ownership and accountability.
Technology platform. Many MedLink members are using findhelp, a public benefit organization with a network of more than 550,000 program locations, to address drivers of health such as food insecurity. Findhelp’s platform allows members to directly connect patients with upstream DOH resources. For example, the platform can help members find resources such as food pantries that provide healthy food to support specific Atrium Health programs such as diabetes prevention.
Outcomes. MedLink members and partners have served more than 89% of the medically underserved population in Mecklenburg County.
Use existing performance measures to understand progress
While conducting program evaluations is often difficult for many CBOs due to a lack of resources, evaluations play an essential role in attracting additional funding and assessing the impact within communities. Interviewees suggested using and building upon existing KPIs, rather than reinventing the wheel. This approach can be helpful because the indicators often are being used for other programs and generally are well-understood. Here are a few ways that CBOs are measuring progress:
- The Magnolia Initiative uses the Early Development Index, a population measure of children’s development at five years of age based on a checklist completed by their kindergarten teachers. The measure comprises over 100 questions that help assess five developmental parameters for assessing school readiness: physical health and well-being,22 social competence, emotional maturity, language and cognitive skills, and communication skills and general knowledge.23
- To revitalize the Uptown neighborhood of Toledo, Ohio, nonprofit health system ProMedica plans to track indicators such as jobs created and emergency department readmission rates for participants in its nonclinical programs.24
- The Project Room Key collaborative partnership in Vallejo, Calif., houses vulnerable people experiencing homelessness in hotel and motel rooms, while also providing medical care and meals. This has been particularly important to slow down the spread of COVID-19 infection. The partners track the number of people housed and COVID-19 infection rates in their county.25
- Technology platforms use search activity to identify how many users are actively logged-in, which nonprofits have signed up on their network, the number of connections to programs, referrals, and referral responses, and the outcomes achieved.
Government’s role in community-based ecosystems
Government agencies at all levels continue to participate in community health initiatives. In addition to being a direct partner, the public sector plays a critical role, particularly in encouraging innovative and sustainable partnerships (see sidebar, “Magnolia Community Initiative,” for more information). For example, CMS has noted that adopting value-based care arrangements in Medicaid and the Children’s Health Insurance Program could help states address health disparities, improve outcomes for vulnerable populations, and reduce costs for the programs.26
The ongoing move toward value-based care is changing the incentive structure for health systems and thereby encouraging more investments in community-based ecosystems. A few other examples of the US government’s participation in ecosystems include:
- Innovative pilots: CMS’s Accountable Health Communities Model is based on emerging evidence that addressing health-related social needs through enhanced clinical-community linkages can improve health outcomes and reduce costs.27 Twenty-eight health care organizations participate in this model that promotes collaboration by screening beneficiaries to identify unmet health-related social needs, referring them to community services, assisting with access to services, and aligning partners to help ensure that services are available and responsive to the needs of the community.
- Funding and reimbursement: Policy shifts that enable the use of funding streams to support collaborative work are important. Whether through grants to new organizations and ecosystems or changes in reimbursement policies, activities such as these can promote and sustain change. For example, in 2016, a modification to Medicaid’s managed care regulation enabled states to pay based on value and outcomes over the volume of services. With the Green & Healthy Homes Initiative, a Medicaid-managed care plan can find a private investor to pay a service provider to address asthma triggers in a beneficiary’s home. Addressing the underlying asthma trigger can result in fewer health issues. The Medicaid plan would compensate the investor with a percentage of the savings achieved due to this intervention.28
- Policy and regulatory changes: Interviewees noted the structural and sustainable impact that policy changes can make on health equity. Cities and towns are making policy changes to promote healthier living (see sidebar, “Blue Cross Blue Shield of Minnesota’s Center for Prevention,” for more information). Project Room Key in Vallejo, Calif. (which provided housing to the unhoused during the pandemic) grew into a statewide program called Homekey that supports permanent housing solutions and is established in state statute with funding from both federal and state governments. However, some regulations continue to hinder health systems from providing support for DOH. Re-evaluating these policies and regulations can incentivize more work in this area.
Blue Cross Blue Shield of Minnesota’s Center for Prevention
Goal: The Center for Prevention at Blue Cross and Blue Shield (BCBS) of Minnesota focuses on improving the health of all Minnesotans by reducing commercial tobacco use and increasing access to affordable, healthy foods. The Center collaborates with other organizations to advance racial and health equity to transform communities and create a healthier Minnesota.
Initiatives:29
- Co-chairing the Minnesotans for a Smoke-Free Generation, a coalition of over 60 community organizations that support policies to reduce youth smoking and to end death and disease associated with commercial tobacco use. The coalition’s four major goals include: keeping commercial tobacco prices high, raising the commercial tobacco sale age to 21, limiting access to candy-, fruit-, and menthol-flavored tobacco, and funding future tobacco prevention programs.
- Assisting Leech Lake Tribal College in setting up a commercial tobacco-free policy on their campus.
- Investing in community-led solutions and collaborations to advance policy, systems, and environmental change.
Outcomes:30
- Minneapolis, St. Paul, Duluth, and Falcon Heights passed ordinances in 2017 and 2018 that restricted the sale of menthol commercial tobacco products to adult-only stores.
- In November 2021, St. Paul, MN passed a set of retail tobacco policies that will help improve health equity, reduce youth tobacco use, and reduce the presence of commercial tobacco across communities in the city. It is currently the most comprehensive price discounting policy in the country as it includes e-cigarettes.
- Members of the Minnesotans for a Smoke-Free Generation coalition testified in support of these bills, which eventually resulted in the Minnesota Tobacco 21 law coming into effect in August 2020, ensuring implementation, compliance, and enforcement of commercial tobacco sale age to 21 years.
Create healthier communities with an ecosystem approach
Community-based organizations and their partners have been working to create healthier communities for many years. These partnerships have directly impacted outcomes by driving policy change and providing housing, food, health care, job training, and a myriad of other services. To build on this ongoing work, community-based ecosystems likely will need additional partners, shared goals, technology, and metrics. But most importantly, it will require the participation and leadership of more community members.
As our case studies show, each community-based ecosystem is uniquely defined by the strengths of its members and the specific needs of its community. Partner organizations can benefit from truly listening to each other and members of the community to understand lived experience and what’s most needed. There’s also an opportunity to learn from the successes—and failures—of other organizations. By working collaboratively with a shared sense of purpose, community-based ecosystems can potentially address multiple drivers of health at once, improve health equity, and move towards the Future of HealthTM, and create the world we all aspire to live in—an environment in which everyone can thrive.
Deloitte's Services for the Health Care Industry
Amid uncertainty and change, health care stakeholders are looking for new ways to transform the journey of care. By focusing on the differentiated needs of plans and providers, our US health care practice helps clients transform uncertainty into possibility, and rapid change into lasting progress. The Deloitte Health Equity Institute, under the guidance of leaders Jay Bhatt and Kulleni Gebreyes, conducts original research and disseminates findings to help drive data-based equitable outcomes, as well as activate interventions that address systemic inequities.
