What the pandemic can teach us about building a resilient public health workforce
Bright spots point to ways that agencies—and workers—can recover from budget cuts and the effects of the pandemic


Matt Garrett

Alison Muckle Egizi

Amrita Datar

Charlotte Sawyer

Jessica Grubbs
Worker commitment shows a way forward for public health
In spring 2020, as millions of Americans were sheltered at home, wrenching TV images came from overwhelmed hospitals, as exhausted doctors and nurses faced a surging pandemic with inadequate supplies and protection. Behind the scenes, exhausted public health workers labored around the clock to keep the novel virus at bay. They ran test clinics, coordinated community mitigation efforts, and led research to improve treatment, develop prevention strategies, and protect the most vulnerable. As citizens applauded health care workers nightly, the daily mental, physical, and emotional strain on many public health workers went unseen.
A de Beaumont Foundation survey conducted between September 2021 and January 2022 painted a fraught picture of the state of the nation’s public health workforce at the local, state, and federal levels.1 Surveyed workers reported symptoms of post-traumatic stress disorder, while their executives mentioned bullying and harassment. Employees at all levels cited the pandemic as a reason for potentially leaving the public health workforce in the coming year.
And those workers may not have fully recovered yet.
Their situation wasn’t ideal even before COVID-19. Between 2017 and 2021, as the fentanyl crisis surged, nearly half of all employees at state and local health agencies quit.2 The influx of pandemic-related funding has ebbed and budgets are tightening once again, exposing the underfunding of public health agencies even as their agendas expand to encompass the well-being of the entire population.3
The expanded agenda and higher stakes, however, have given public health greater workplace meaning. Nine in 10 public health employees feel their work is important and say they’re determined to give it their best efforts every day.4
Public health organizations are leaning into the broader agenda, increasingly looking to work across sectors to implement a whole health approach involving innovative partnerships. Such partnerships to modernize data systems and improve constituents’ social and environmental conditions are already bearing fruit.
Moreover, the composition of the workforce has changed dramatically. As Dr. Betty Bekemeier explained during a recent conference panel presentation, the workforce composition is becoming more diverse in terms of age, race, and lived experiences—shifts that can fundamentally change public health practice and research for the better.5
Agencies are creating new roles, redesigning benefits, and providing employees with new skills. These efforts signal a unique opportunity to rethink how the broader US public health system operates—how to make it more resilient both during normal operations and in times of crisis, and how to provide better support for the current and next generations of public health workers.
Budgets are expected to remain an ongoing challenge, and agencies undoubtedly will face fresh problems in the coming years. But while much of the public health workforce remains committed to its cause—the question is how to maintain and expand that commitment.
In this report, we share bright spots from public health leaders and considerations for rethinking the boundaries of the public health profession. The bright spots that these leaders highlight not only help bring our suggestions to life but also offer a sense of optimism in challenging times.
Keeping the conversation healthy and aspirational
The public health field is deeply familiar with “thinking in systems” to address complex challenges and identify policy solutions, acknowledging that health is influenced by factors beyond medical care, such as where we live, work, and play. Health and wellness have become shared societal aims, moving the work of public health beyond agency walls.
Systems thinking can help chart a path forward. For instance, in 2021, the de Beaumont Foundation estimated that the nation’s public health services needed to attract and retain some 80,000 new employees just to cover essential services. Meeting that demand would likely require collaboration across the entire ecosystem and involve all available resources.6 Public health leaders should understand the talent ecosystem and partner with foundations and other stakeholders to place professionals where they’re needed most.
This report takes this prevailing approach and pairs it with a positive, appreciative, inquiry-style data collection method to study the strengths and virtues that enable individuals and communities to thrive. We identify bright spots for individuals, teams, and organizations across government levels, highlighting a potential path toward greater resilience and asserting the importance of centering diversity, equity, inclusion, and accessibility in all efforts.
Methodology
This report synthesizes findings from a series of interviews with leaders from the public health profession and academia (see Appendix). These interviews emphasized how programs at the local, state, and federal levels are applying lessons from recent public health responses to bolster the workforce. Spotlights throughout the report are based on interview discussions.
Lessons from the pandemic: Four ways to activate the public health workforce ecosystem
Collaboration and flexibility stand out as common themes of bright spots in the public health domain. The challenges agencies faced during the COVID-19 pandemic showed that networks and coordinated partnerships can be more effective than individual agencies. Leaders also saw how flexibility—in how and where work is done, in funding mechanisms, and in hiring—can unlock creativity and new, often better ways of operating.
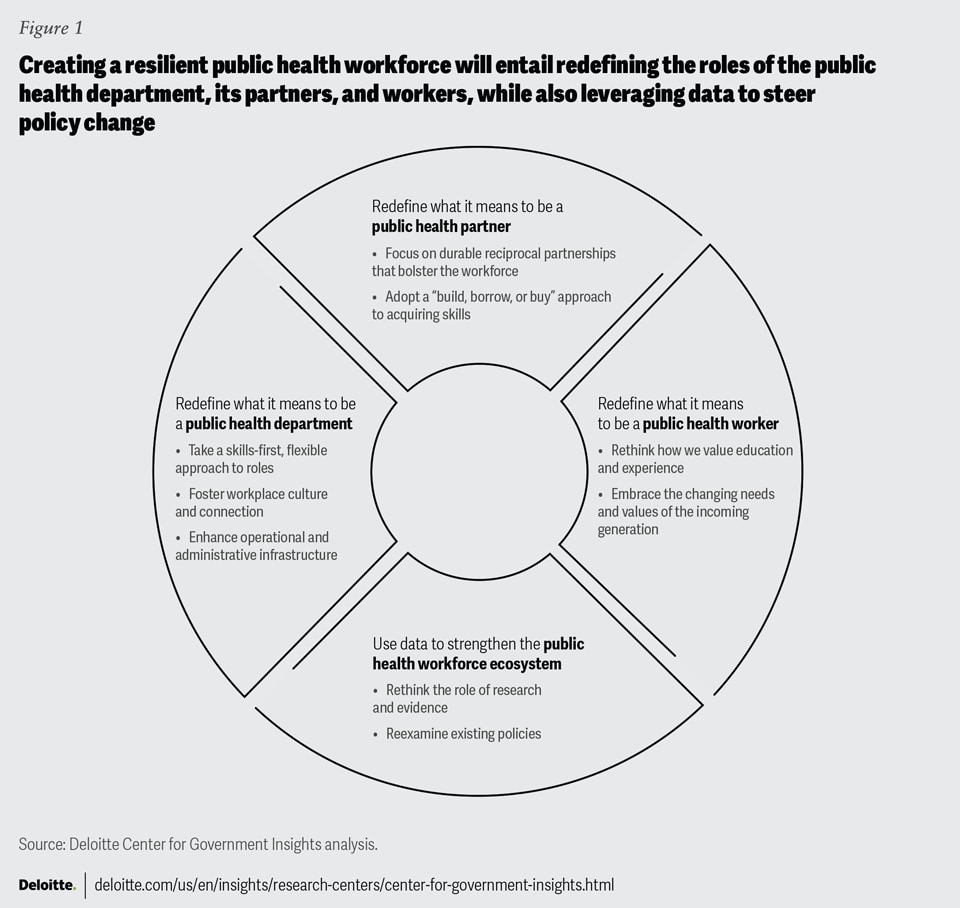
Here are four steps that can help build a more resilient public health workforce (figure 1).

1. Redefine what it means to be a public health partner
In the words of Public Health Institute CEO Mary Pittman, “We are all public health.”7 The public health domain includes an ever-expanding range of organizations and skills beyond urgent care and epidemiology. Agencies are seeking employee experience in areas including data science, communications, public relations, social media, user experience research, design, psychology, counseling, behavioral science, social work, environmental science, and nutrition. Other, less tangible skills—such as compassion, empathy, trust-building, persuasion, community relationships, and lived experience—also play a key role.
External relationships in the public health ecosystem are relatively new, and many actors are still learning their roles. Yet in the long term, enduring partnerships across the ecosystem could pay off, supplementing the workforce and improving constituents’ health and quality of life. Partners can draw new and diverse skills to the field to tackle the growing list of activities that comprise public health.
“Public health lacks influence, it lacks credibility, and often it lacks resources. It needs to be in coalitions, it needs to work with others to succeed.”
—Michael S. Sparer, JD, PhD, professor and chair of the Department of Health Policy and Management, Mailman School of Public Health at Columbia University
Focus on durable, reciprocal partnerships that can bolster the workforce
Public health entities at all levels of government are expanding their use of partnerships, looking to local businesses and community organizations for support with messaging and collaboration on activities during health emergencies. Durable relationships often require continuous engagement with communities and businesses. And these relationships should be reciprocal—partners that have something to gain may be more likely to stick around.
The Colorado Public Health Workforce Collaborative is a statewide partnership of 20 organizations including health care providers, hospitals, public health departments, and educational leaders.8 Initially created to ramp up contact tracing during the pandemic, it now focuses on developing innovative approaches to address urgent challenges such as widespread workforce burnout. Through a partnership with the University of Colorado Department of Psychiatry, the group has led regular small-group therapy sessions for local health directors, as well as recovery-focused sessions local health directors can use as forums to build staff resilience and support healing.9
The group has also trained more than 1,400 contact tracers, led a statewide analysis evaluating local agency messaging strategies, and established a data collection strategy to evaluate needed workforce resources and monitor workforce shortages.10 Its workforce development action plan focuses on equitable recruitment and retention, career pathways, and useful workforce data.11
Adopt a “build, borrow, or buy” approach to skills acquisition
Ideally, an organization can build the skills and capabilities it needs by training its own staff. It can also “buy” the desired capabilities, with new hires if the need is ongoing or through contractors for short-term needs. Or it can “borrow” talent through rotations, internships, or special projects or sharing workers with specialized skill sets (such as data scientists) that provide skills that are hard to find, difficult to train, or too expensive to hire permanently.
Partnering across the public health ecosystem can help supplement recruitment efforts, as with the hiring of contact tracers during the pandemic. Local health offices can collaborate with hospitals, health systems, and technical schools. In North Carolina, for instance, the Burke County health department has a partnership with a two-campus, 275-bed hospital, sharing health care employees on a part-time basis to boost agency capacity.12
Departments might consider using partnerships to:
- Match the right skills to the appropriate roles. The public health field requires both soft and technical skills. Partnerships can help match individuals and organizations with the roles or tasks that support the best possible mutual outcomes. For example, people with local experience and strong community ties often can work well in specific communities to drive behavioral change. Agencies can partner with state labor departments to identify registered community health-worker apprentices or work with local community-based organizations to identify candidates for community-based roles.
- Capitalize on multiple academic partner pathways. Capstone programs in public health often require graduate theses developed through hands-on work in the field. Graduate public health students can drive research and evaluation projects that suit both their academic goals and agency priorities, saving the agency from hiring additional full-time research staff. Medical professionals with dual-faculty appointments in academia and public health settings can lend provider resources at a lower cost. Community colleges can also consider partnering to build public health accreditation experiences for people with skills like data science, advanced computing, and artificial intelligence, skills that are not traditionally taught in public health. (For an example of fellowships driving hiring, see “Spotlight on New York: Bolstering infrastructure through fellowships.”)
- Collaborate with hospitals and health systems to tap resources for community health needs. In some communities, organizations can collaborate with area hospitals on assessments of local health needs, rather than working independently toward similar aims. If state health departments already lead in this work, they could play a convening role. Community and faith groups can serve in an advisory capacity, lending assistance and expertise.
- Use shared-services arrangements across the ecosystem to recruit new talent. Such arrangements can allow jurisdictions and departments to pool resources for various activities such as recruitment campaigns targeted at public health careers.
- Share recruitment leading practices and success stories. To attract more talent to the public health field and nurture a healthy pipeline of workers, ecosystem partners can share leading practices and successful hiring tactics to bring more people into the field.
Spotlight on New York: Bolstering infrastructure through fellowships
The New York State Public Health Corps Fellowship Program, founded in 2021, aims to bolster state and local public health infrastructure by recruiting diverse talent. Program coordinators work with local and the state health departments to recruit for the specialized skills they need from nearby schools. For example, if a department needs public health nurses, the program can ask local nursing schools to promote the fellowship program and encourage people to apply upon graduation. The coordinators have also established relationships with community-based organizations to increase public awareness of professional opportunities.
“If you can think of a public health program, we probably have a fellow working on it.”
— Erin C. Knoerl, assistant director, New York State Public Health Corps Fellowship Program
Program fellows take a public health–essentials course and gain practical experience in the field through the program that places fellows in local health and state department roles across the state to respond to current and future emergencies, thus building applicable skills. The goal is for fellows to move into full-time employment in public health.
The program hasn’t been without challenges, however. Some local health departments chose not to participate; others have been troubled by the fact that fellows’ salaries may exceed those of their own employees.13 Still, the fellows were able to fulfill important roles, supporting emergency points of dispensing and administering medical countermeasures, vaccination, and testing sites, and assisting with local and state programs that had been sidelined due to the pandemic, such as those dealing with maternal and child health. The program has hired and placed 507 fellows to date and currently has 319 active fellows.14 Some fellows have moved into permanent positions with state or local departments.15
2. Redefine what it means to be a public health department
One of the most pressing challenges facing today’s public health leaders is how to attract and keep their employees engaged in an environment of tight budgets and elevated levels of stress and uncertainty. Listening to the needs of the workforce is an important step. Responding to these needs can involve several leadership strategies, such as adopting a “skills-first” approach, fostering workplace culture and connection, and bolstering operational and administrative infrastructure.
Take a skills-first, flexible approach to roles
During the pandemic, agencies recognized the power of having a more fluid workforce with a skills-based approach, which enabled them to accomplish more with limited resources. (For an example of how interoperability can drive efficiencies, see “Spotlight on Ashland County Health Department: Workforce interoperability for maximum efficiency.”)
Spotlight on Ashland County Health Department: Workforce interoperability for maximum efficiency
Many health departments faced the challenge of delivering their services with limited staff and highly restrictive working conditions during the pandemic. By taking a fluid approach to skills and the tasks they needed to accomplish, Ashland County’s department was able to mobilize its staff in creative ways.
Its leaders listened to staff members who believed they had underused skills and, with some spot training, put them to work in new roles. For instance, recognizing that environmental health staff members weren’t visiting restaurants due to the shutdown, someone from that team took over managing and sharing information on social media. Someone else tackled phone calls and figured out how to structure and analyze incoming complaints.
The department has since worked these alternate skills into its emergency response plans. “As a small department, we’re already wearing multiple hats, but now we can fine-tune that a little more,” notes Health Commissioner Vickie Taylor.16
To build a skills-first workforce, health departments should:
- Understand in-house skills. Knowing your people’s competencies beyond the ones connected with their day-to-day work can be highly useful. Central organizations can create “pods” of such talent that can be deployed when and where they’re most needed.
- Foster skills across the organization. Organizations can train “interdisciplinary” employees who can move into new roles as needs evolve. This can also benefit workers looking to diversify their experiences. One way to do this is to offer rotational programs giving new hires experiences across the organization.
- Approach work on a “jobs-to-be-done” basis. By viewing work tasks in terms of the outcomes or goals they’re meant to accomplish, departments can expand the options available to get these jobs done—for example, by deciding whether to use partnerships, recruit new workers, borrow talent through rotations and fellowships, or hire contractors.
Foster workplace culture and connection
Any organization’s culture is the sum of its shared values, traditions, attitudes, and, most importantly, behaviors. In today’s new world of work, organizations should look to intentionally curate and define their workplace cultures. Leaders can build an environment of mutual trust and shape culture by focusing on the factors most important to workers, such as belonging (the feeling of connection with a group or community), well-being (including mental health and access to education, resources, and training), flexibility (giving employees a sense of control and ownership over their work by holding them accountable without micromanagement), and purpose (reminding them they’re part of the larger mission no matter what their role).
Health departments can:
- Lead by example to shape team behavior. Agency leaders and managers should model the behaviors they wish to encourage within the organization. For example, during a conference panel, a former director of the Massachusetts Department of Public Health described how she made regular thank-you calls to express appreciation for employees’ work.17 Even such small gestures can boost worker morale and feelings of connection with their teams. Practices that emphasize a mission focus and strengthen teams, such as sharing success stories or recognizing people’s contributions, should become the norm.
- Promote inclusion and belonging. More workers are seeking inclusive workplaces. Highlighting an organization’s inclusive culture during the hiring process can help attract diverse candidates—for example, by using gender-inclusive language in job postings or adding personal pronouns to email signatures.
Enhance operational and administrative infrastructure
To help boost retention and recruitment, public health departments should ensure that they have the right systems, processes, and resources to support their workforce goals. These could range from hiring processes and training resources to data-sharing practices and employee well-being initiatives—all vital components in building a positive employee experience and cultivating resilience within the organization. In addition to in-house capabilities, departments can tap into resources from the broader public health ecosystem, including the Association of State and Territorial Health Officials (ASTHO) (see "Spotlight on ASTHO's PH-HERO initiative" for more details) and NACCHO, for planning and leadership training.18
Spotlight on ASTHO’s PH-HERO initiative
ASTHO launched its Public Health—Hope, Equity, Resilience, and Opportunity (PH-HERO) initiative in winter 2022 to support health officials and their staffs in countering worker burnout and stress. The initiative began as a pilot with five participating jurisdictions and is expected to expand; it also includes a publicly available resource center for public health leaders.19
PH-HERO works with public health leaders to identify agency-specific issues that can be addressed through focused planning and supports them with leadership development training, such as trauma-responsive leadership, which focuses on how to foster employee well-being in the context of repetitive workplace trauma,20 learning supervisory training, and coaching. In this manner, PH-HERO enables changes to help enhance agency staff’s everyday work experience.
Some practices that can support hiring and workforce goals include:
- Targeting recruitment to the needs of key groups. Different groups, for example, millennials or baby boomers, have unique priorities and needs. Organizations can identify the types of employees they want to hire and tailor recruitment strategies, benefits structures, and available roles and job postings accordingly.
- Skills-tracking and credentialing. Health departments should share a common language or taxonomy to standardize skills, and an accompanying credentialing system to share skills data.
3. Redefine what it means to be a public health worker
A shift in the educational credentials and experience required to be a “public health worker” is already under way, as community health workers are increasingly viewed as a department’s most valuable assets. The rise in importance of demonstrated skills and empathy has increased the need for community health workers, especially in areas such as substance abuse and harm reduction.21 At the same time, at least 16 US states have dropped degree requirements from some public sector jobs, signaling an openness toward a skills-first approach to hiring.22
Thinking more broadly about skills and roles can help boost readiness in “normal” and emergency situations alike. It can help agencies by encouraging them to hire for harder-to-train skills such as empathy and then offer new hires training in public health and technical skills.
Rethinking how we value education and experience
Today, public health entities should consider rethinking and redefining the roles and skills they need to attract passionate, committed individuals, with or without public health degrees, to join the field (see “Spotlight on Public Health AmeriCorps” for an example).
Some programs aim to bring in whole new groups of people into the field.
Spotlight on Public Health AmeriCorps
The federal Public Health AmeriCorps, launched in fall 2022, offers opportunities for individuals ages 17 and over, with no higher degree or public health experience required.
The program offers its fellows onsite experience and financial assistance for future careers in health and medicine while focused on advancing more equitable health outcomes for underserved communities.23 It recruits workers according to grantee needs, placing fellows to work in a wide range of areas such as outreach and education, aid for survivors of domestic abuse, sexually transmitted disease–testing, and recovery care for opioid-use disorder.
During a recent conference panel, one fellow shared that she’d had to abandon a nursing degree while her parents were both sick and she was caring for two children. She was able to use the AmeriCorps education award to complete her degree: “My experience has been lifesaving.”24 Another fellow we interviewed said she would never have considered working in the field; Public Health AmeriCorps helped her realize that “public health is not work that is done behind the curtain—instead, you are impacting millions of people.” She intends to pursue a career in public health.25 The program already boasts many success stories, with nearly 4,000 members recruited and with plans to expand its reach and impact.26
“This unique partnership between CDC and AmeriCorps leverages CDC’s expertise as the nation’s leading public health agency and AmeriCorps' connection to local public health and volunteerism across the country. It’s bringing a whole new group of people to an experience in the public health field.”
—AJ Pearlman, director, Public Health AmeriCorps
To expand their focus on skills, organizations should:
- Assess the competencies certain roles truly need. For some roles, should soft skills or lived experience be prioritized over formal credentials? Can degree requirements be relaxed in some areas? Can some skills be learned easily on the job? A clear understanding of such themes can help reshape hiring policies to encourage more workers to join the field.
- Create pipelines for older workers seeking “second acts.” Older, seasoned talent can be attracted by partnering with local businesses and national corporations. Many baby boomers, as they ease into retirement, are looking to pursue a second act—and often one driven by their values.27 Such individuals can fill a myriad of public health roles, leveraging their skill sets, and help build a cadre of “accredited gig workers” who can pick up tasks and shifts when needed.
- Establish core competencies, but don’t let certifications be a barrier to entry. Public health professionals, with their diverse range of skills and roles, often don’t require credentialing to begin work in public health. But employees can acquire additional skills related to their role that can improve the field. There’s a benefit to ensuring a sufficient level of public health knowledge among data scientists, communications leaders, policy advocates, and health care employers looking for reliable training and preparedness. Public health core competencies can help define the skills and development programs needed for different roles.
Embrace the changing needs and values of the next generations
Organizations across public health often recruit college or even high school students as interns or fellows, introducing them to the public health field. It’s proven to be a mutually beneficial relationship, due to the inventiveness and innovation young people can bring to the table.
Fresh thinking can help attract new talent to public health based on what matters most to them. A 2022 Deloitte Global survey of 22,000 millennial and Gen Z respondents found that these groups prioritize remote and flexible work options, career advancement opportunities for part-time workers, mental health support, job stability, and opportunities to address social and environmental issues.28 In addition, they have high expectations for their businesses’ societal impact; fewer than a quarter of respondents felt satisfied with that of their employers.29 Public health already shines in many of these areas.
“We need to listen to the younger generation and give them an opportunity. I think this next generation is better educated than my generation was, is more innovative, and will be more of a help going forward.”
—Danny Scalise II, MBA, MPH, director, Burke County Health Department
On the heels of the COVID-19 pandemic, agency leaders are responding to an increased desire for flexibility through remote and hybrid jobs. They’re seeking creative solutions for the challenges employees face while balancing work with caregiving and other responsibilities.30 Many also offer opportunities for tuition assistance and reimbursement, partner with academic institutions to offer continuing education opportunities, and provide mentoring and professional development.
To expand the pool of public health workers, organizations should:
- Shape benefits structures around the needs and desires of the groups they are trying to attract, focusing on what matters to them. Nontraditional benefits such as in-vitro fertilization, adoption leave, and on-site childcare appeal to many recruits. Another compelling benefit is loan repayment assistance to help offset the cost of the education often required to break into the field of public health. Future research could investigate benefits priorities through collective listening by states, higher education, and public health programs.
- Support workplace mental health. High-stress environments such as public health are well-suited for workplace mental health resources and benefits that signal concern about employee well-being. Health departments can facilitate connections to such resources across the ecosystem.
- Offer flexible working options based on employee input. Many of today’s workers want flexibility and a better work/life balance. Where applicable, a degree of flexibility in work hours and locations can make public health jobs more attractive. Seek staff input to help design flexible schedules with employee needs in mind, such as nonnegotiable childcare pickup schedules.
- Adjust hiring processes to suit remote roles. Person-to-person health work remains essential, especially in rural and smaller health departments where community knowledge is a core job competency. But specialists like data scientists, whose work is typically conducted independently on computers, may be good candidates for remote work.
4. Use data to strengthen the public health workforce ecosystem
Partnerships can be crucial to ensuring that research-driven evidence shapes public health policy and guidance as well as workforce decisions.
Reexamining existing policies
Policy and legislative changes can improve workforce outcomes, and agencies in a position to educate policymakers should prioritize it. Leaders should consider partnering with private organizations that can work with policymakers more directly.
Specific policy areas to reconsider include federal and state investments in recruitment efforts, competitive pay structures, state hiring caps and rosters, civil service requirements, and accreditation standards.
To help further policy changes supporting a stronger workforce, public health leaders should:
- Build policy skills into standard training. The next generation of leaders should be fluent in policy. Departments should support such training for staff members and work with schools of public health to create more professional development opportunities.
- Work across the ecosystem to influence decision-making. When agencies can’t directly educate policymakers, partnerships can help, especially for workforce issues. For example, agencies could consider collaborating with the National Governors Association and other national-level policy groups that can lend resources to improve the hiring infrastructure.
- Seek widespread input on crucial issues. Garner input early and often from state leaders as well as local health departments. During the pandemic, Indiana’s governor traveled around the state to hear from local departments about their workforce needs and was able to finalize a US$255 million public health funding package with enough flexibility for local adaptation.31 The bill specifies 60% of funding should be spent on new priority health areas for the state. The legislature was not restrictive in providing how those funds should be spent.32
- Partner with universities to promote executive non-degree programs for mayors, county commissioners, and others. Spreading basic public health knowledge can go a long way in forwarding the needs of the workforce. Elected officials lacking public health training or awareness may, for instance, assume health care and public health are one in the same. Universities offer customizable non-degree health policy programs that could be tailored to political partners.33
Rethinking the role of research and evidence
Strong research is important to support and improve the public health workforce. One step for the research agenda is to increase response rates for recurring surveys of health departments. In a 2022 national profile of local health departments, only 38% of departments responded to the survey, compared to 76% in 2016.34 When professionals don’t see such data being used to generate meaningful guidance, they may be less likely to participate, and the less they participate, the less likely professional associations and even government leaders may be willing to invest in additional workforce research.
Still, recent progress is encouraging. In 2023, the University of Washington conducted a survey of rural health departments focused on workforce experiences and needs that achieved a 40% response rate and great interest from those surveyed.35 In 2022, the University of Minnesota’s Center for Public Health Workforce Research received funding from the Health Resources and Services Administration for six researchers as part of a consortium to carry out small workforce studies.36 This sort of funding is new, and more should be considered.
Funding flexibility
Public health organizations across the nation face challenges both from insufficient resources and limitations on the use of existing funds.37 Designing public health workforce funding for maximum flexibility can help organizations to address their workforce needs more effectively.
“We need to allow people to be creative with how they spend funding,” says Ashland County health commissioner Vickie Taylor. “We are having a hard time spending some of our COVID-19 dollars because they are so restrictive. It’s difficult to spend when we could reallocate it in a way that would really help. By the time the money gets to you, you’re already past the crisis. We need more leniency with what we can use funding for.”38
The Public Health Infrastructure Grant: Flexible funding for the public health workforce
The Public Health Infrastructure Grant overseen by the US Centers for Disease Control and Prevention (CDC) gives health departments flexibility in investing in workforce, foundational public health services, and data modernization. “The number one thing we are learning,” says CDC senior adviser Steve Reynolds, “is that health departments need flexible funding to be able to choose what they need when it comes to workforce.”39
Using funds from this grant, the State of Ohio Association of Health Commissioners, in 2021, established a student loan–repayment program supporting the state’s local health departments. The association handles the administrative tasks, allowing even small departments to offer loan repayment as a benefit.40
Rebuilding the workforce through partnerships — and listening
By blending the tenets of systems thinking and positive, appreciative inquiry-style data collection, this report identifies numerous bright spots that underscore the value of using an ecosystem approach to strengthen the public health workforce, at a time when that workforce is in need of support. New and expanded partnerships can offer mechanisms for scaling recruitment efforts, allowing more people with diverse skills and educational backgrounds to find a professional home in public health.
Our interviews also highlighted ways to strengthen the public health workforce ecosystem. Though it may seem obvious, listening to what the workforce wants is critical, particularly as many public health agencies prepare for an exodus of tenured professionals and seek workers from younger generations.41 Flexible funding mechanisms in public health help agencies to meet the needs of the current workforce and ready the field for future demands. Changes to benefits structures and other policy changes in service of public health workers likely deserve further exploration.
Our research calls for the need to rethink the role of public health education and experience, and to expand the evidence base to establish what works in sustaining a resilient public health workforce. These opportunities for future inquiry bolster the case for continued, collective action across all elements of the public health workforce ecosystem. Let’s continue to chart the path forward.
Appendix: Interviews with sector leaders
This report is based on a combination of interviews that took place between July and November 2023, and secondary research. Individuals interviewed represent federal, state, local, and nonprofit organizations throughout the country (see table).











{kind=link}
{kind=link}