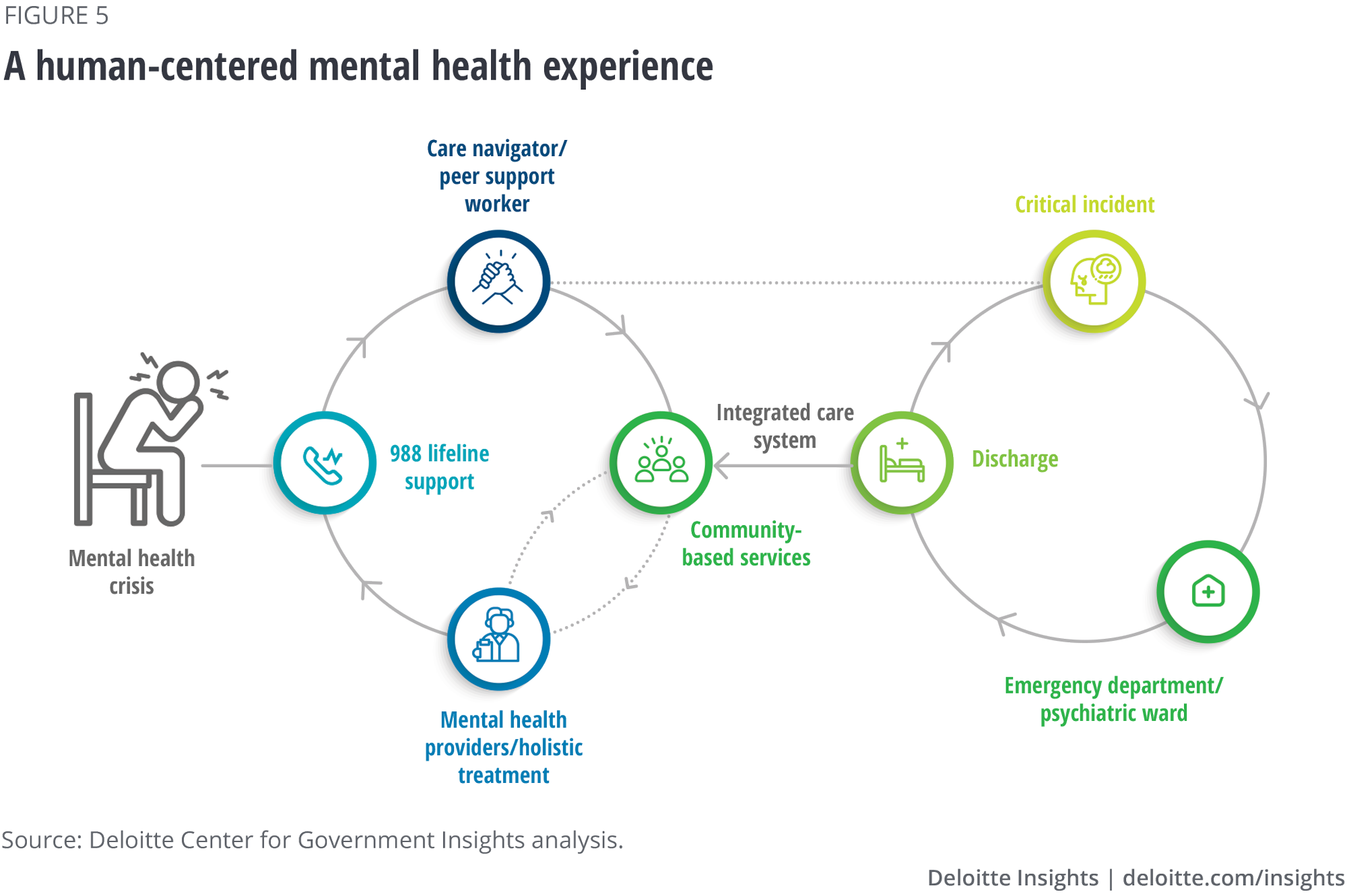
We synthesized the findings to develop a human-centered vision for the mental health ecosystem, reinforced by the efforts already underway by state, local, and federal health leaders. This vision hinges upon five major shifts for better mental health care access:
- Expand the mental health workforce by augmenting loan repayment programs and other incentives to inspire professionals to serve in areas where there is a provider shortage while investing in community mental health training programs, encouraging greater workforce diversity, and exploring engaging retiring providers as resources.
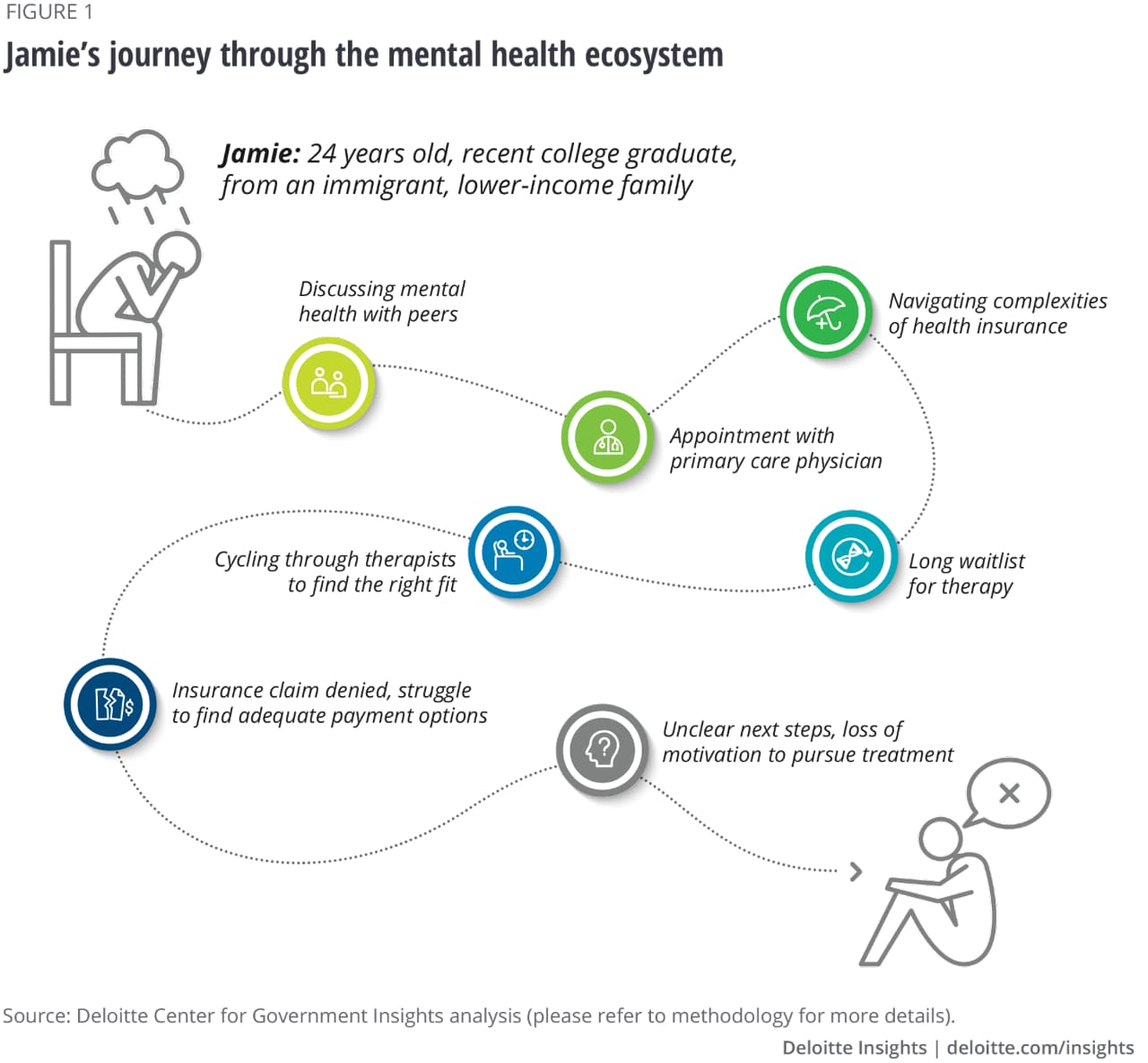
- Transform the user navigation experience to meet people where they are, building upon shared data systems for tracking local mental health needs, creating archetypes of individuals’ mental health journeys as models for design-thinking, developing a digital mental health crisis support platform, funding ecosystem care navigators, and bringing human-centered design to mental health care insurance coverage.
- Catalyze the development of recognized, innovative models, such as integrated behavioral and primary care models, clubhouses, mobile and home-based care, and in-community services like library-based social workers.
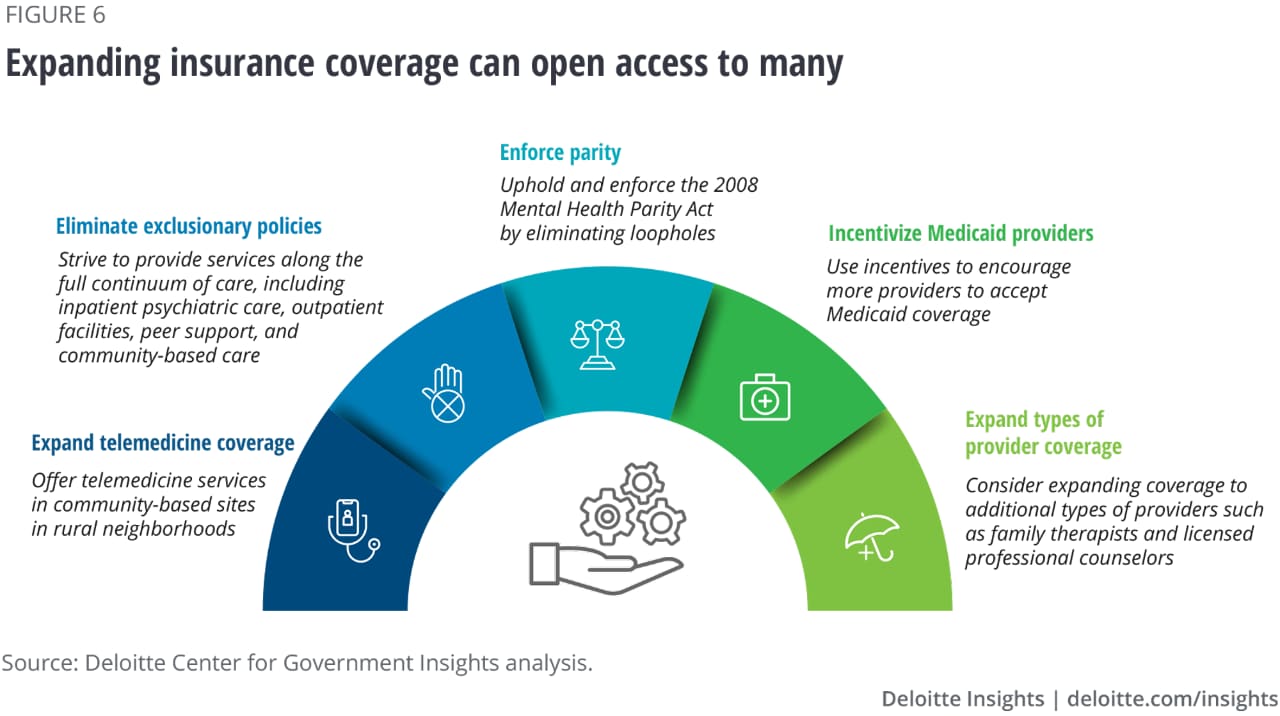
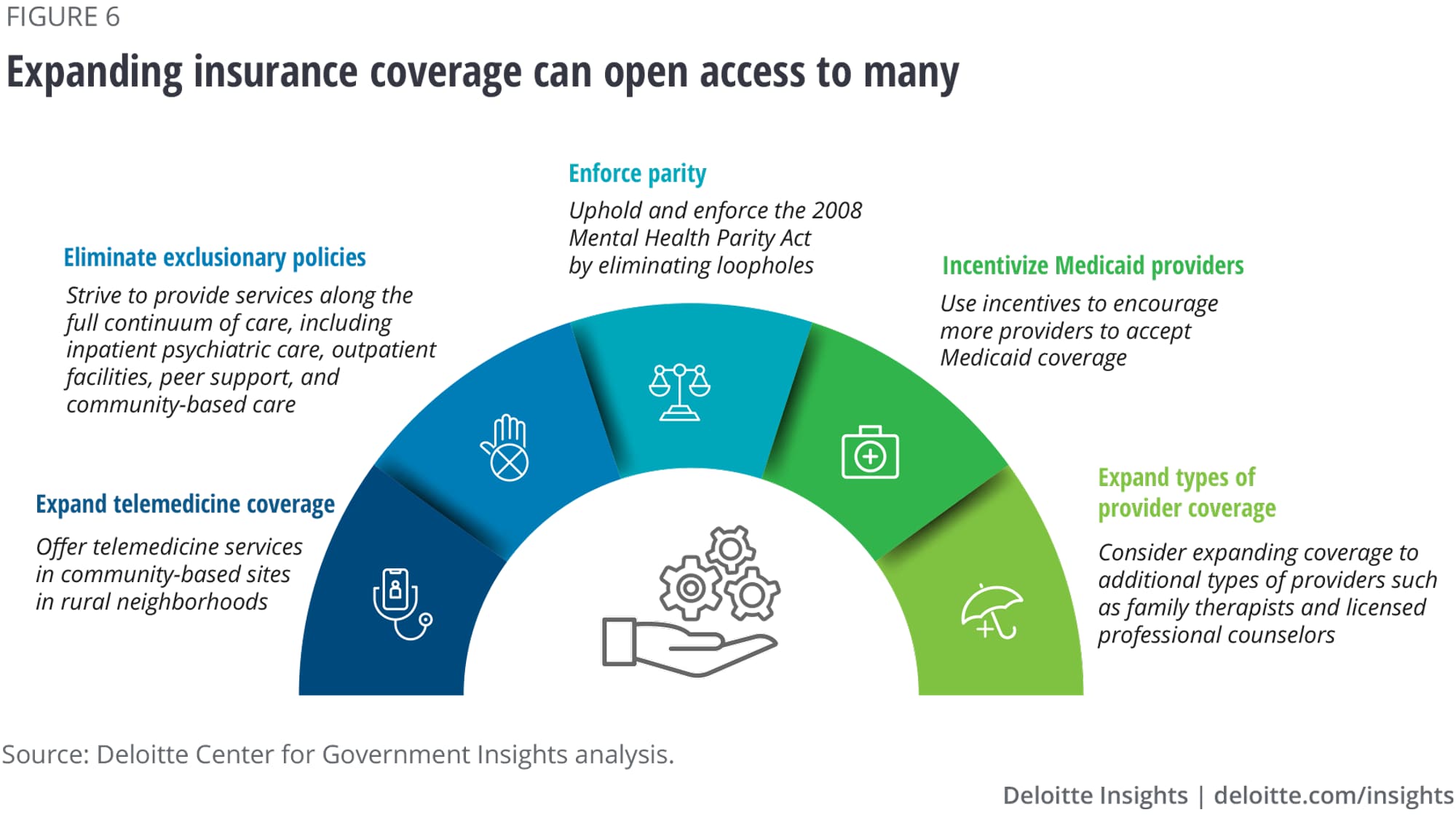
- Increase public and private insurance coverage by continuing to refine the regulatory framework, remedying exclusionary policies, expanding Medicare and Medicaid telemedicine coverage for adults, and incentivizing more providers to accept Medicaid coverage.
- Reform payment systems by working with insurers to reduce burden of excessive paperwork on providers, supporting alternative payment models, and making it easy for providers to serve individuals seeking care across state lines.
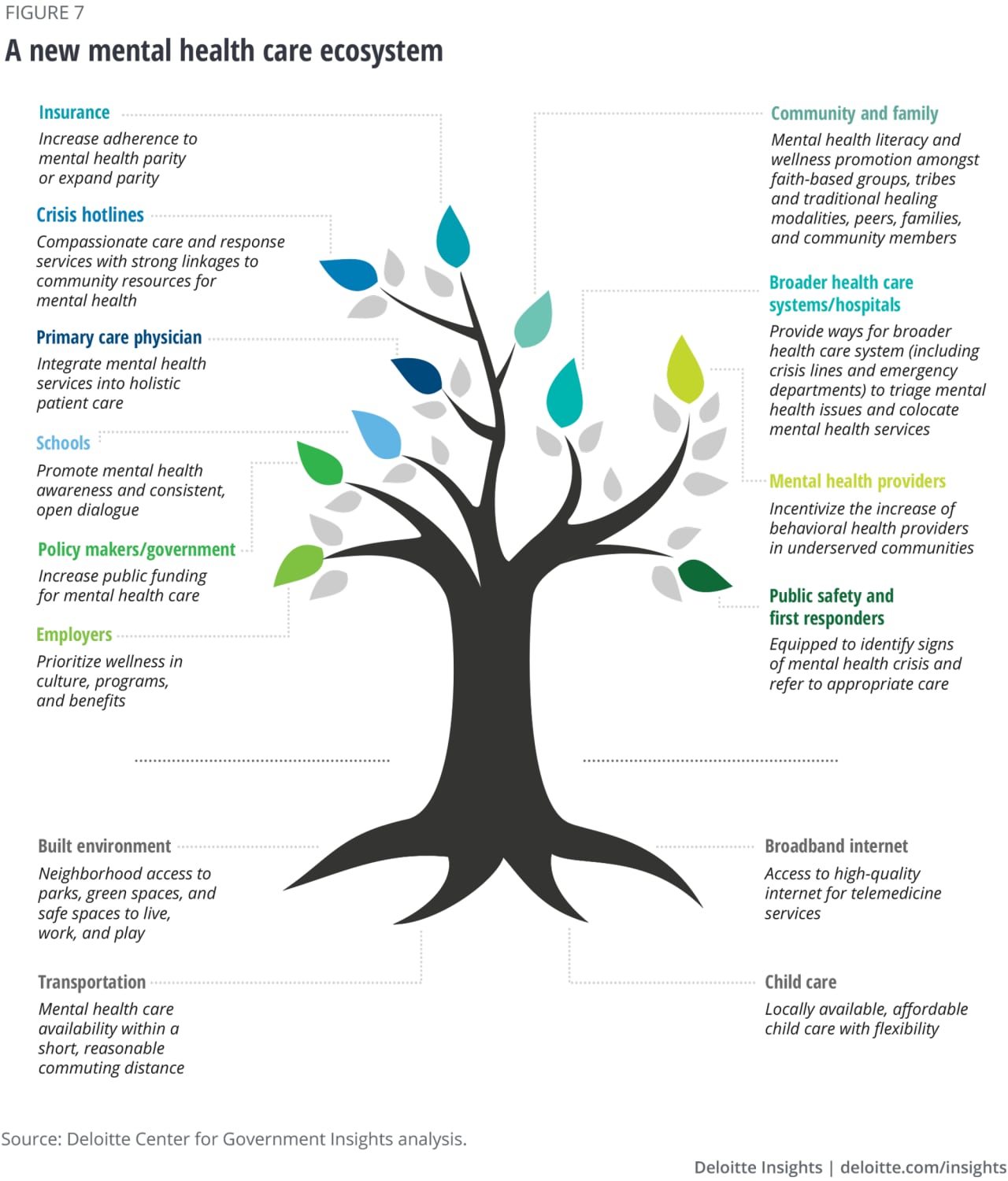
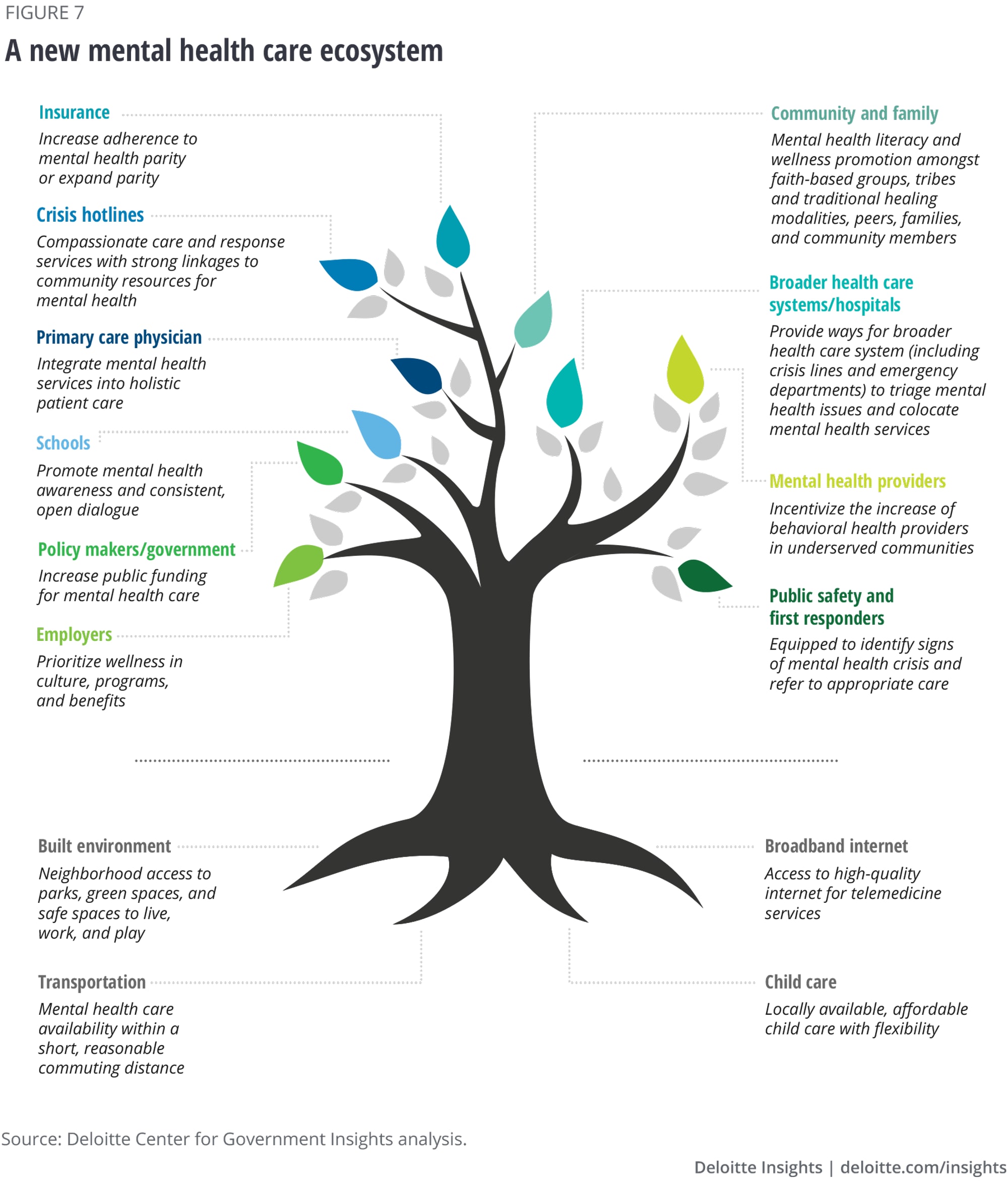
With these shifts, a new mental health care ecosystem is imaginable, a coordinated system in which all actors work in tandem to offer compassionate care in an easy-to-navigate, affordable, equitable, and nonstigmatizing system.
Policymakers, federal health agencies, state, local, and community authorities and providers can collaborate to build the infrastructure and support necessary to meet people where they are with the services they need.
Together with investments in prevention and early intervention, these proposed shifts can help create a nation in which every American has the opportunity to thrive.
The current mental health situation
Rates of mental illness across the globe are climbing, prompting a global call to action to strengthen mental health care.1 According to the World Health Organization (WHO), the worldwide incidence of mental illness and substance abuse disorders rose by 13% between 2007 and 2017.2 The situation has only been exacerbated by the pandemic, economic dislocation, and strife over the years since.3 Over the first year of the pandemic, there was a 25% increase in the prevalence of anxiety and depression globally.4
Nearly 50 million adults in the United States experienced some form of mental illness in 2022, and more than half of them received no treatment for their conditions.5 In 2020, there was a 30% increase in emergency department visits for mental health amongst 12–17-year-olds.6 Mental illness among the youth has risen to the extent that it is considered by many mental health care professionals to be a national emergency. Yet only 20% of teens with mental health needs have received mental health care.7
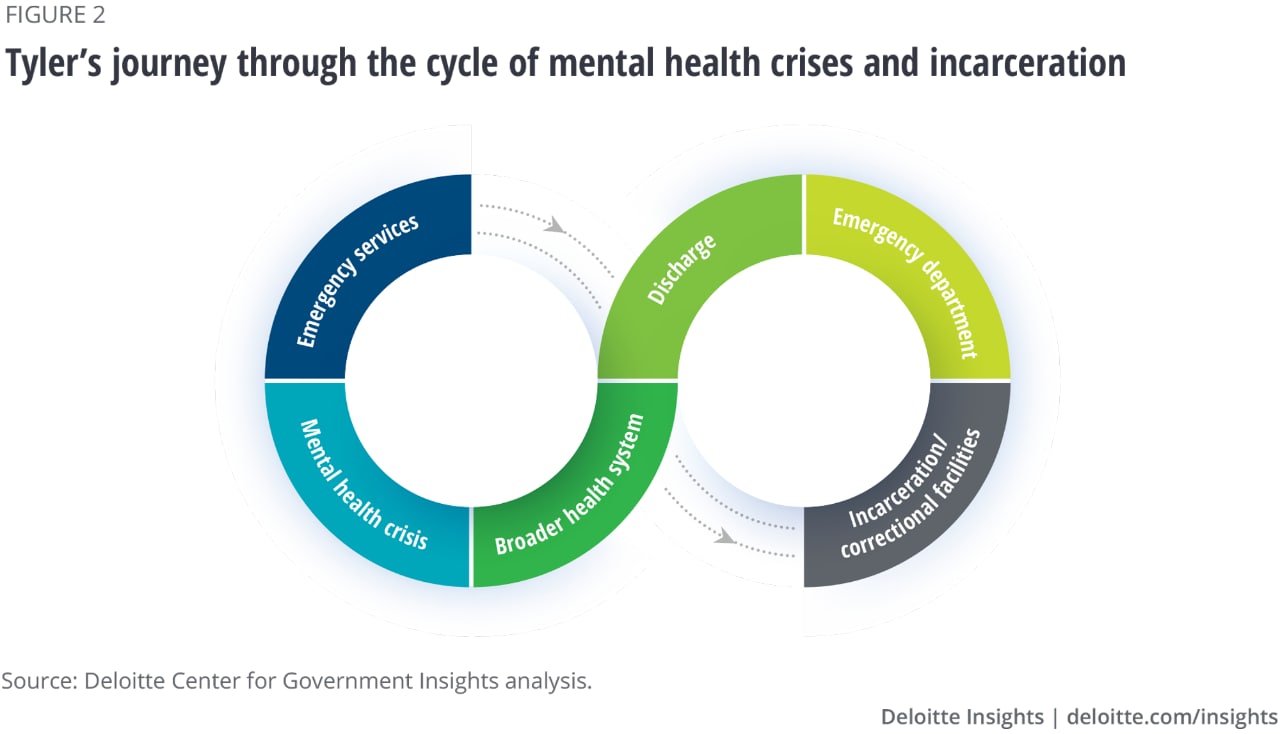
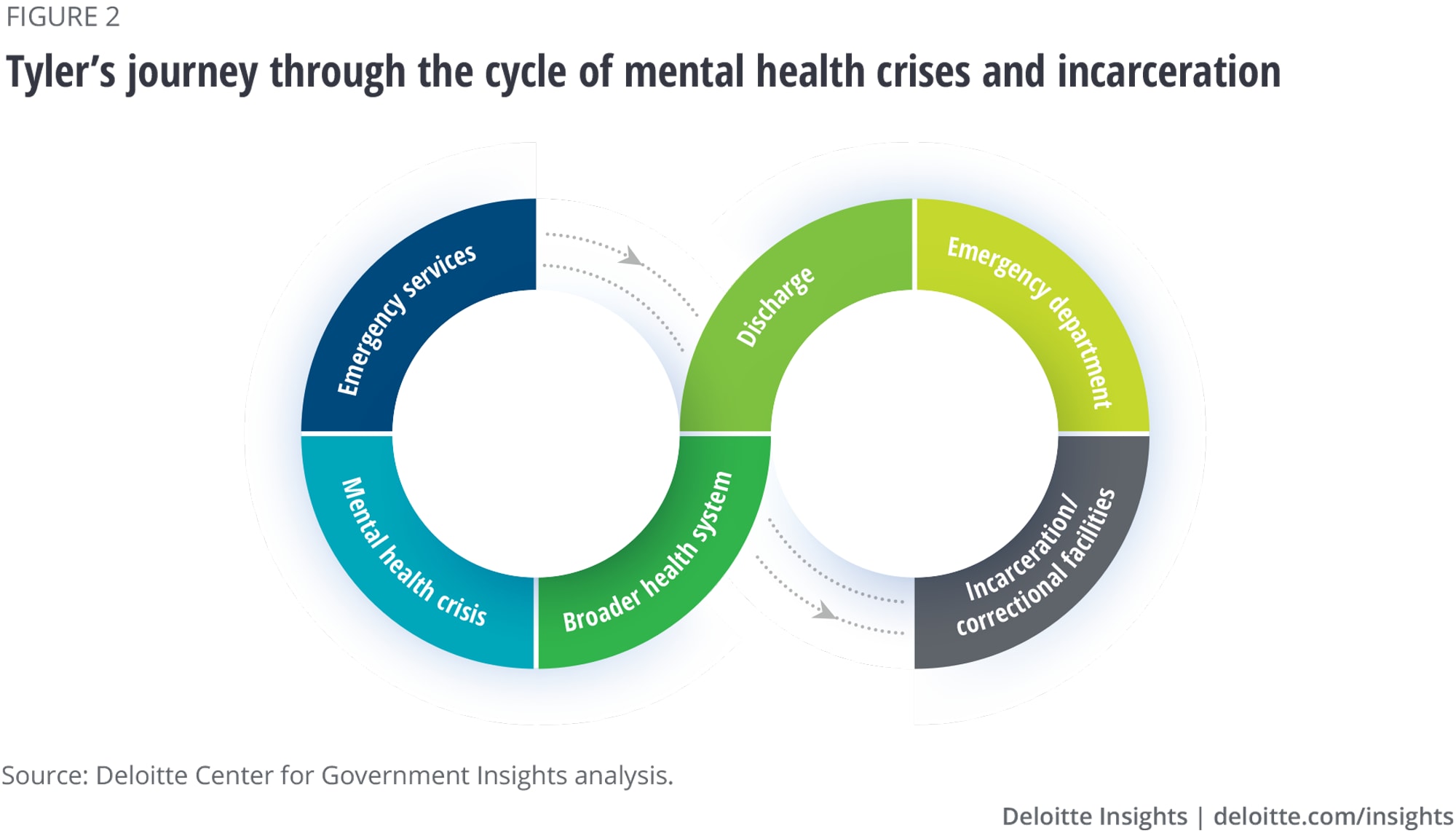
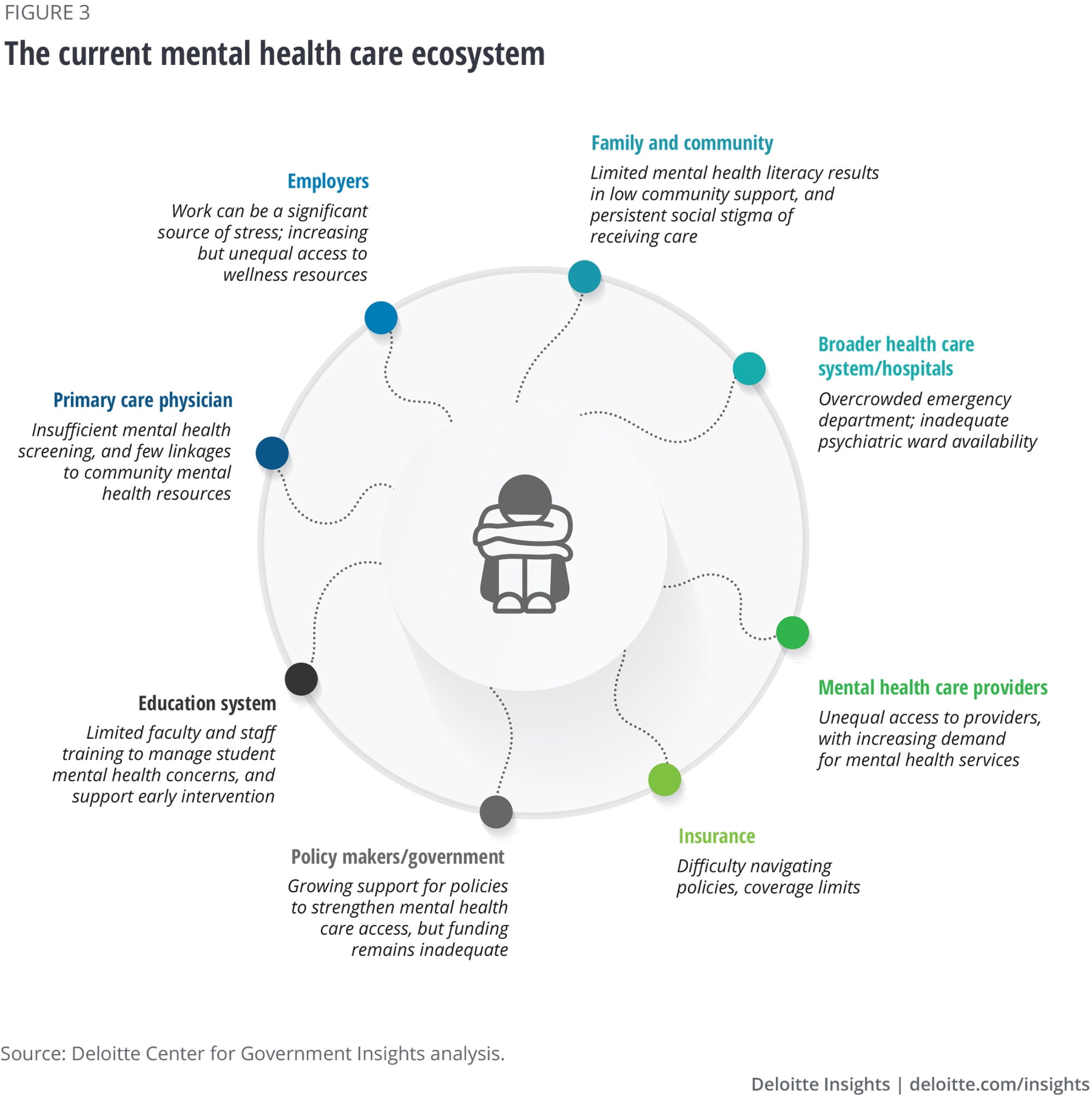
The current mental health situation in the United States and other countries grew from decades of public stigma, government inertia, and a broken care ecosystem.8 Navigating our mental health system can require a level of patience and persistence that can be difficult to muster when one is in distress or crisis. Further, individuals with severe mental illness who are also experiencing housing insecurity can find themselves in near-constant transition between group homes, psychiatric wards, emergency rooms—and the street.9 It can be challenging to secure stable support.
Access can be further reduced by limited availability of mental health providers in some areas of the country—along with high out-of-pocket costs. Access to mental health providers is uneven across the United States, with 37% of the country living in a mental health provider shortage area, which are areas with one or fewer mental health professionals per 30,000 residents.10 Two-thirds of those shortages occur in rural or partially rural areas. As of September 2021, 96.4% of Wisconsin residents and 80% of Mississippi residents live areas where there is a shortage in mental health providers.11 Conversely, only 4% of Massachusetts residents and 0% of Vermont residents live in such areas.12 Where available, mental health care is unaffordable for many. The Substance Abuse and Mental Health Services Administration reports that high costs prevented nearly 44% of Americans with any mental health issues and up to 52% of adults with serious mental illness from receiving treatment in 2019.13
Mental health care access has a direct impact not just on those experiencing mental illness and their families, but also on governments and the broader economy. Untreated mental illness can lead to diminished productivity, higher unemployment, foregone tax revenue, higher welfare expenditures, and an increase in physical ailments such as cardiovascular and metabolic disease.14
Still, addressing mental health challenges can yield substantial returns. According to the Lancet Global Health Journal, “for every US$1 invested in scaled-up treatment for depression and anxiety, there is a US$4 return in better health and productivity.”15 The Biden Administration’s prioritization of mental health marks a milestone toward an improved system that can provide enhanced access to those who need mental health care.16
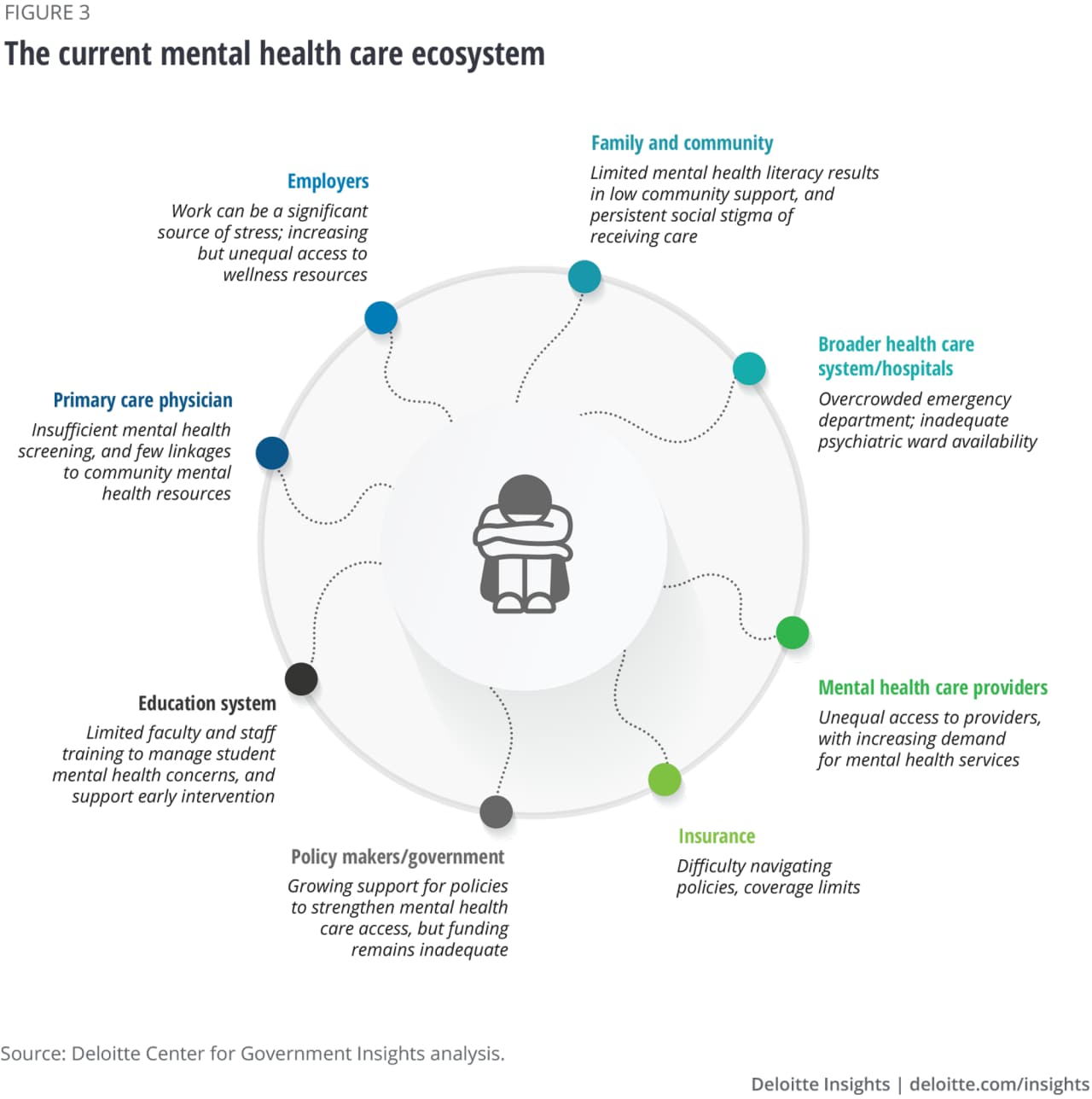
Importantly, improved care access is just one component of a multipronged strategy to create a better mental health system. Mental health is shaped by who you are (such as biology, socioeconomic status, race, gender, marital status, and employment status), who you are with (such as peers, family, community members), and where you live. Factors such as neighborhood poverty, crime, racism, and housing quality can influence mental health, in addition to work and school conditions.17 Children who experience early trauma may have worsened mental health over their lives.18 Investment in protective factors—such as improved neighborhood conditions, affordable housing, job opportunities, safe spaces for community connection such as parks and churches, and wraparound early childhood supports—can go a long way toward improving the current mental health situation.19
In this report, we share findings from our research on the challenges and opportunities inherent in navigating our current mental health care ecosystem and propose five shifts to create a more accessible US mental health care system for all.



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}