The projected costs and economic impact of mental health inequities in the United States
If left unaddressed, mental health inequities could lead to about US$14 trillion in excess costs between now and 2040, according to our analysis
Daniel E. Dawes
Jay Bhatt
Nelson Dunlap
Christian Amador
Kulleni Gebreyes
Brian Rush
Mental health inequities may not only harm individuals but also hinder economic prosperity.1 To gain a broader understanding of the costs associated with mental health inequities in the United States, the Deloitte Health Equity Institute and the School of Global Health at Meharry Medical College conducted an equity-focused quantitative analysis. The study examined various types of expenditures related to mental health inequities that have not been explored in detail in other literature, ranging from chronic physical ailments like diabetes and hypertension to productivity-related losses stemming from absenteeism and unemployment (see methodology).
Projecting to 2040: US$14 trillion in excess spending
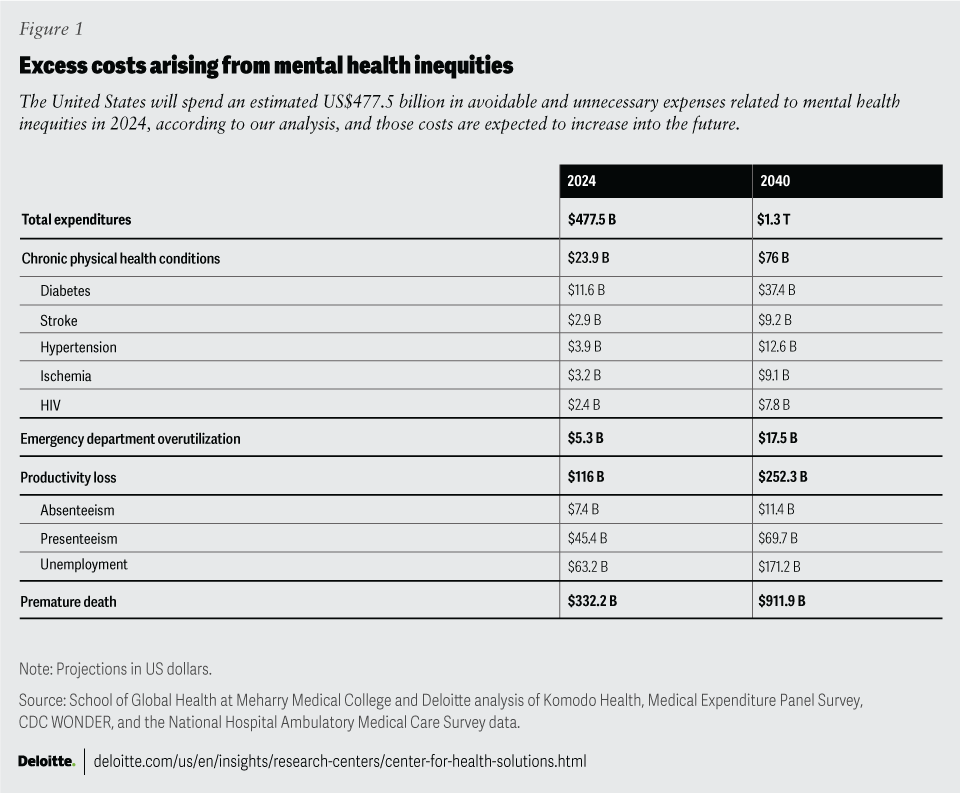
Across the expenditures measured in this analysis, excess costs arising from mental health inequities total an estimated US$477.5 billion in 2024 (figure 1). The measured trends indicate that costs will continue to grow through and beyond 2040, when excess spending in these categories alone is likely to exceed US$1.3 trillion, with cumulative costs by that time totaling nearly US$14 trillion. This equates to a cost to society of roughly US$42,000 per person living in the United States.
Addressing equity in mental health is an important factor underpinning any success society will have in reducing inequities in mental health, improving chronic physical health disease management, and curtailing the rise of excess health spending. We examined the evidence to determine if it is possible to reduce the impact of mental health inequities, and if so, where leaders can find the most leverage to do so. This report emphasizes the importance of understanding the future mental health status of the United States and its impact on health and health care spending.
What gives rise to higher mental health prevalence rates?
This analysis utilizes prevalence rates as an indication of how common or prevalent mental health-related conditions are among distinct populations in the United States and the cost placed on individuals and society as a result of inequities in those rates. This analysis is not intended to fully identify the underlying causes of those prevalence rates. However, previous research has shown that political and social determinants of health cause an often-unfair distribution of resources and opportunities, resulting in risk factors that are beyond the control of the individuals on whom they act.2 It is well-documented in research that demographic factors such as race and ethnicity are not risk factors in and of themselves.3 However, political processes, societal structures, and social conditions contribute to variances in disease incidence for these groups, as well as outcomes for individuals experiencing those disease states.4
By prioritizing equity in mental health policies and practices and understanding the political determinants of health framework outlined in this report, leaders across diverse sectors could unlock significant economic benefits while helping to foster a healthier, more resilient society, and remove the economic burden that Americans may bear if society allows mental health inequities to compound.5
Who is most affected by the cost of mental health inequities?
The economic burden of health inequities has increased over the years, as indicated by various studies. Although the burden of mental health conditions in the United States continues to grow across all demographic groups, certain populations such as racial or ethnic minority groups, the justice-involved community (including incarcerated individuals, parolees, etc.), people living with disabilities, members of the LGBTQIA+ community, low-income individuals, and many others, have historically experienced challenges at a rate that is unsettlingly high.6
- Although the White population shows the highest prevalence of mental health diagnosis, it is non‐White populations that tend to bear more of the cost associated with mental health struggles. This is likely due to the long-standing structural racism and the legacy of policies that disadvantage certain populations, as well as social and economic conditions.
- In general, higher prevalence of mental health conditions and higher prevalence of other chronic conditions are correlated. Lower-income populations with mental health challenges have higher prevalence of other chronic conditions. Issues such as lack of access to care and cultural stigma mean that this report likely undercounts—rather than overcounts—individuals with mental health challenges.
- Groups with mental health challenges account for more workdays missed and have a higher rate of unemployment than those without such challenges. For those with mental health conditions, higher prevalence of other chronic conditions, more days missed from work, and higher unemployment are seen across all age groups.
Methodology
To gain a broader understanding of the economic burden of mental health inequities in the United States, the School of Global Health at Meharry Medical College and the Deloitte Health Equity Institute conducted an equity-focused quantitative analysis of data from Komodo’s Healthcare Map,7 the Medical Expenditure Panel Survey from the Agency for Healthcare Research and Quality, the Centers for Disease Control and Prevention’s WONDER database, and the CDC’s National Hospital Ambulatory Medical Care Survey. This analysis expands on the methodology used within Thomas LaVeist, Darrell Gaskin, and Patrick Richard’s health disparities research described in the 2009 report, The Economic Burden of Health Inequalities in the United States.8 While previous analyses have quantified the impact of mental health on productivity, they have not attempted to quantify the cost due to inequities specifically. Quantifying productivity lost as a result of inequities in mental health outcomes by race and ethnicity enabled this analysis to achieve a nuanced view of the interconnected relationship between mental and physical health.
This report begins to quantify the disparities in outcomes—and the potential cost of mental inequity associated with those disparities—related to four different types of costs.
- Chronic physical health conditions: Potentially avoidable medical expenditures related to the intersection of mental health inequities and physical health outcomes
- Emergency department utilization: Medical expenditures related to untreated or undertreated mental health conditions that resulted in avoidable emergency department utilization
- Productivity loss: Economic cost resulting from loss of productivity in the workforce due to mental health conditions
- Premature death: Economic cost resulting from deaths due to suicide, deaths associated with substance use disorders, deaths due to inadequate mental health treatment, and deaths due to mental illness associated with comorbid illnesses
Click here to download the full version of the report, which highlights disparities experienced by three key population groups, segmented by race and ethnicity, socioeconomic status, and age. Although other populations experience inequities in mental and behavioral health like those found in this study and are deserving of similar research that focuses on their circumstances, this report can be seen as a small window into a large issue. Other population segmentations were considered, such as populations based on gender and sexual orientation, but due to data limitations they were ultimately not included as part of our initial analysis. The exclusion of other populations should not be misunderstood as an assessment of their importance, nor of the likely scale of mental health challenges among those groups. In fact, this report should be taken, in part, as a catalyst for additional research into additional populations.
Similar to the research approach utilized by Thomas LaVeist, Darrell Gaskin, and Patrick Richard in their analysis of the economic burden of health inequities, for each analysis, a “baseline population” was identified to highlight the inequities that exist across races and ethnicities, socioeconomic statuses, and ages.9 This baseline population is identified as having lower prevalence rates of chronic conditions, fewer days missed at work on average, or the lowest unemployment rates when compared across groups. This report proposes, based on the literature and original research, that, for groups experiencing higher incidence of chronic conditions compared to the “baseline population,” the gap that exists is impacted by mental health inequities. The hypothesis is that, with attention to the political and social determinants of health as well as increased access to equitable care, treatments, and supports, all prevalence rates, number of days missed from work, and unemployment would closely align with the baseline population. As a result of these lower incidences of chronic conditions, fewer missed days at work, and lower unemployment, the potential dollars that could be saved are calculated related to closing this gap.
Chronic physical health conditions and the associated cost of mental health inequities
Mental health is the invisible counterpart to physical health. Previous studies have revealed that a person’s mental health can impact their physical health and vice versa.10 Therefore, this study aims to quantify those who are suffering from concomitant chronic physical health conditions and mental health conditions, and when inequities exist to determine who is bearing more of the burden of disease.
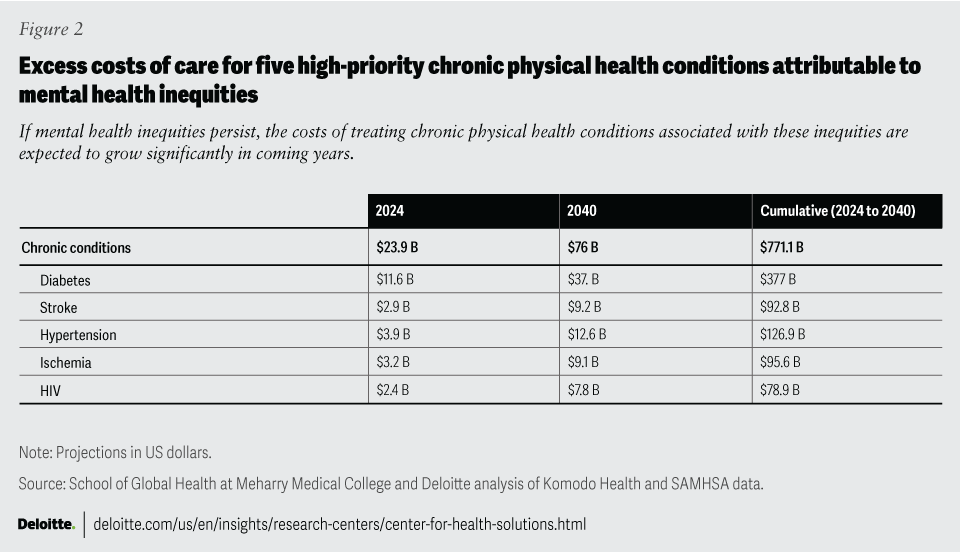
The analysis shared in this report identifies the estimated cost of five high-priority chronic physical health conditions associated with excess spending that may be attributable to mental health inequities (figure 2). Diabetes, cardiovascular disease (including stroke, hypertension, and ischemia), and HIV were chosen due to their prevalence, cost to society, and known or suspected links to mental health.11 Download the full report for more insights into the physical health conditions highlighted in this analysis, including variations and disparities across populations.
The intersection of mental health inequities and emergency department utilization
One consequence of inequitable health care is the excessive reliance on the emergency department (ED) for mental health–related incidents and the overall overuse of the ED by individuals facing mental health challenges.12 This can not only result in higher direct costs but also an increased burden on health systems’ limited capacity and leads to increases in wait times for other patients.
In our analysis, we looked at data on frequent users of the ED, which we defined as individuals who had five or more mental health–related ED visits in a single year. By analyzing additional health care interactions, such as inpatient visits following an ED visit, the full scope of costs and health care utilization becomes visible, suggesting the true scope of the potential avoidable costs that result from inadequate and inequitable mental health care.
US$5.3 billion
Estimated costs due to emergency department visits associated with mental health inequities in 2024
US$17.5 billion
Projected annual costs by 2040 if left unaddressed
The analysis demonstrates that nearly half of the individuals who frequently use the ED also experience mental health challenges, irrespective of their initial reason for seeking care. These trends are highly suggestive that with appropriate access to mental health care, a large portion of the ED visits for these chronic users could be avoided. Whereas patients with appropriate access may schedule a visit with a primary care physician or behavioral health specialist, populations that lack that level of access may be more likely to use the ED as both their primary care service and mental health service as it is open 24/7, does not require a prior appointment, and in general, has fewer barriers than primary care to see a physician.13 Comprehensive mental health care has the potential to not only enhance individual outcomes but also alleviate the burden on emergency health care services.
The intersection of productivity loss and mental health inequities
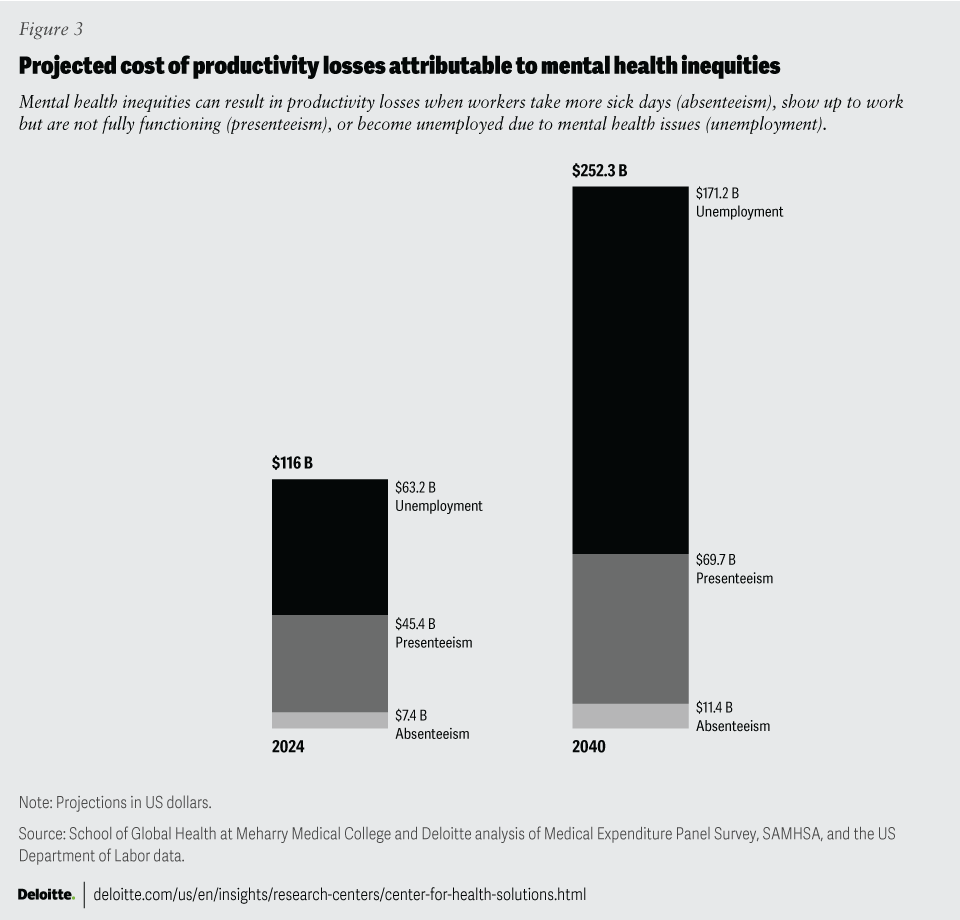
Previous research consistently finds substantial productivity losses attributable to mental health conditions.14 According to the same source, depression is a major contributor to workplace absenteeism, with affected individuals taking more sick days compared to their non-depressed counterparts.15 Presenteeism, the phenomenon of being present at work but not fully functioning due to mental health issues, is another significant factor reducing productivity. Additionally, mental illness can lead to disability claims, resulting in prolonged periods of reduced or lost productivity and additional insurance costs. There is a considerable economic impact of mental health conditions on productivity in the workplace, and an equal value to society of eliminating mental health inequities (figure 3).
Data limitations
Quantifiable wage data and surveys are unlikely to show reliably the potential ripple effect of mental health challenges throughout family groups. For example, when one’s spouse or child struggles with inadequately treated mental health challenges, does the stress on their partner or parents at home translate into fewer productive workdays?
The economic burden of mental health inequities associated with premature death
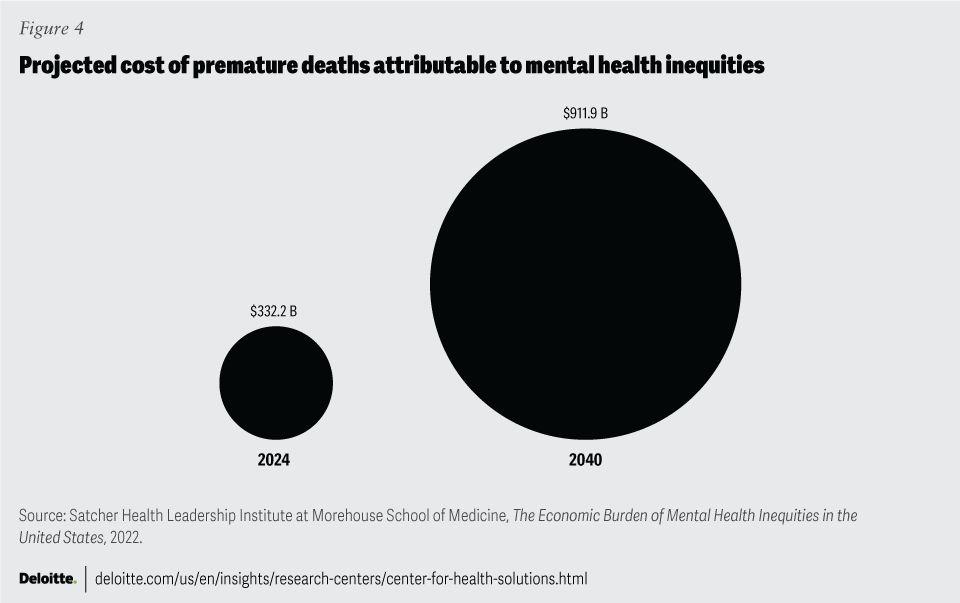
Previous research, highlighted in The Economic Burden of Mental Health Inequities in the United States Report, suggests that premature deaths related to mental health inequities resulted in an estimated cost of US$278 billion between 2016 and 2020.16 This analysis included deaths due to suicide, deaths associated with substance use disorders, deaths due to inadequate mental health treatment, and deaths due to mental illness associated with comorbid illness.
The resulting projection from our analysis estimates that costs have risen, topping US$292 billion in 2022, and they are likely to continue to rise unabated until the growth in premature deaths can be reversed. If the trend remains unchanged, the annual cost of premature deaths in 2040 is projected to reach US$911.9 billion (figure 4). The direct path to reducing premature deaths should account for inequities—especially mental health inequities—that could impact certain populations dying prematurely at greater rates.
Using political and social determinants as a tool for cost containment
As awareness that health is influenced by myriad factors beyond genetics, behavior, and personal decisions has spread, it’s important to recognize that the dilemma of cost containment cannot be fully addressed by the health industry alone. To positively impact population health and individual health outcomes, addressing access and pricing of health care delivery and services is important. But to do so, efforts from many sectors should be aligned to help leverage our understanding of the political and social determinants of health.
While this report builds upon previous efforts to quantify the economic costs of mental health inequities by examining additional indirect costs and comorbidities, it addresses only a subset of each. The costs projected would likely increase dramatically if, for example, physical disability, or many other health conditions, were considered. A more inclusive investigation could become even more complicated as other variables such as political, social, and environmental factors—each of which can be perceived as stressors impacting mental and physical well-being—should be considered.
Yet, many of these stressors are, in the present day, unquantifiable. This leaves us to understand that actuarial science may never be able to fully calculate a final and true cost of inequities at an individual or societal level. In addition, while this report attempts to quantify the inequity-related “costs” of mental illness, suffering, and death, it also respects and understands that there is no dollar figure that can be placed on the value of human life.
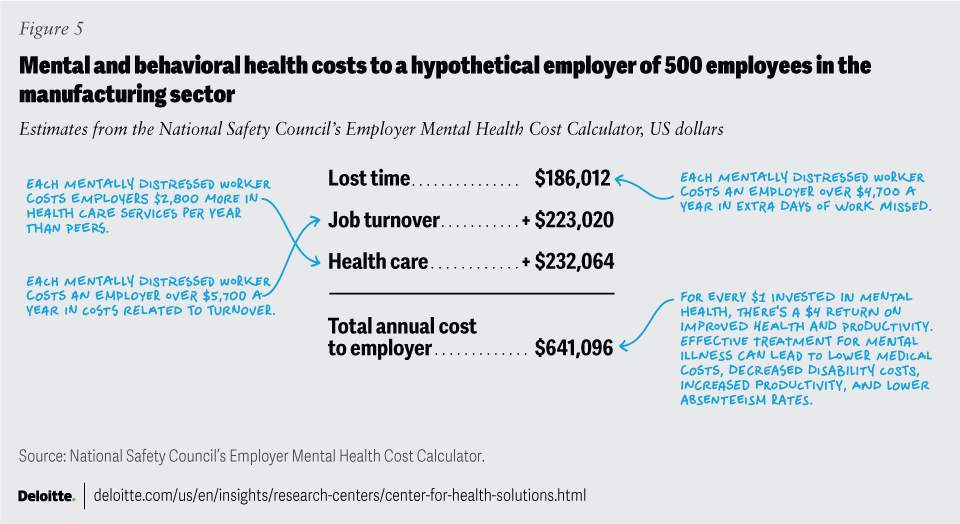
The business costs of mental health inequities for employers
The economics of the issue are as compelling as the moral argument. For example, decreasing health inequities could lower health plans and system costs associated with poor health outcomes that lead to more emergency room visits, longer hospital stays, and unnecessary hospitalizations. This in turn could generate value for the businesses that pay for health care as well as state and federal agencies and the people they serve. Improving health outcomes could also improve quality ratings of both plans and providers, making them eligible for higher payments from Medicare and other value-based care programs designed to reward quality. In the future, we will likely see value-based equity programs that reward not only improvement in average outcomes but also parity of outcomes among different populations.17
Inequities in mental and behavioral health among employees pose significant challenges to both individual well-being and workplace productivity. As demonstrated in this report, poor mental health among employees can significantly impact productivity, especially through both absenteeism and presenteeism. Absenteeism leads to direct costs for organizations. Presenteeism further compounds these costs by reducing overall efficiency and output. Additionally, previous Deloitte research revealed that talent-related issues, including mental health concerns, are major challenges for organizations.18 Leadership behaviors, organizational design, and work practices influence employee well-being, encompassing mental health support as an important component.19
An industrywide trend of prevention and well-being underscores that, for organizations, tangibly advancing health equity can be a point of competitive advantage. Not only can it help them attract leading talent and elevate their brand and reputation, but healthier workers also have fewer sick days, are more productive on the job, and have lower medical care costs.20 Previous Deloitte research shows that employers that prioritize human sustainability in turn foster increased opportunities for employee-led innovation and productivity.21 Expanding workplace benefits and programs to address mental health needs, adequately and equitably, can give organizations a competitive edge. From promoting mental health awareness to providing access to counseling services, supporting mental well-being can be beneficial.22
Reducing medical expenditures associated with mental health inequities
Fiscally responsible leaders in both government and business should find it necessary to reduce health care delivery costs. Demographic and cost trends indicate that spending will rise rapidly between now and 2040 as the populations that are disproportionately burdened grow in comparison to the baseline population. Our analysis reflects that mental health is likely implicated in the incidence and exacerbation of other high-priority chronic conditions—representing both a key challenge and an easy target for reforms that can reduce both inequities and costs. Although equity-centered initiatives will require additional targeted spending, the data indicates that achieving mental health equity can lead to the avoidance of the significantly higher burden that results from the need to manage a growing population of patients with inadequately treated mental health challenges and other chronic diseases.
Medical expenditures are projected to grow an average of 5.4% from now until 2031, based on projections from the Centers for Medicare and Medicaid Services Office of the Actuary.23 However, utilization and medical expenditures for mental health are anticipated to grow at a higher rate. Data reveals an annual increase of 11.5% in mental health services for privately insured individuals from 2019 to 2022, which relates to a 15.4% annual increase in spending on mental health services among privately insured individuals within the same time period.24 Although mental health accounts for only about 5% of overall medical spending, this portion is increasing.25
Deloitte predicts a break in the cost curve for medical expenditures, reducing health care spending between now and 2040—resulting from advancements in disease prevention, detection, and treatments; emerging technologies (increased data-sharing and interoperability); and consumers being highly engaged and empowered.26 However, it will likely require a concerted and cross-sector effort to cause a parallel disruption to effectively reduce the current trajectory of the expenditures associated with mental health inequities identified within this report (Deloitte’s research paper, “Six assumptions for measuring health disruption,” offers insight to inform actions for the business sector).27
The path to mental health equity
The mental health crisis in the United States should be treated as an emergency encompassing a cross-sector approach. Progress should include the active and voluntary participation of the private and commercialized industries that directly or indirectly affect the service and delivery of mental health services.
Large gaps in the incidence rates of mental health conditions—and related chronic physical health conditions—between populations represents major opportunities for leaders to make changes to improve productivity, reduce costs, and enhance the quality of life. Taken separately, any one of these improvements could justify the effort and investment necessary to achieve mental health equity. However, the uniting of these benefits is what makes this a significant issue that should be addressed. Mental health inequities may be addressed and improved by:
- Academia generating research and evidence to advance culturally informed care delivery in clinical training
- Fields of medicine and public health entities recruiting promising clinicians to mental health disciplines and helping to establish integrated care models and centers, which could increase access to care and treatment
- Employers providing culturally informed mental health and well-being resources for an increasingly diverse workforce
- Elected officials providing the political appetite and will to influence policy for the greater good
- Local governance distributing providers and other resources to the places where they are most needed and least found (such as neighborhoods characterized by a high mental health need and high social polarization) to help address the social and political determinants of health that influence mental health inequities
An equity-focused approach to mental health is paramount for our collective prosperity. The inequitable distribution of mental health challenges not only inflicts unnecessary suffering on affected individuals but also imposes substantial direct and indirect costs on society. Therefore, this report operates from the understanding that achieving mental and behavioral health equity can lead to benefits such as improved health outcomes for all members of society suffering from chronic diseases, reduced incidence of those diseases, greater productivity, significantly reduced unnecessary health care spending, and an overall increased well-being.
Appendix 1: Understanding frequently used terminologies within this report
Mental health conditions, challenges, and illnesses are frequently used interchangeably to characterize conditions that affect an individual's thinking, feelings, behaviors, or mood.28 For the purposes of this report, the terms mental health and behavioral health are often used interchangeably, or in tandem, to highlight their close-linked nature and accurately reflect the literature.
Mental health equity is the right of all individuals, regardless of race, age, ethnicity, gender, disability, socioeconomic status, sexual orientation, or geographical location, to access high-quality and affordable mental health care services, and addresses systemic factors driving health inequities.29
Political determinants of health encompass the systematic process of structuring relationships, distributing resources, and administering power that collectively impact health equity.30 These include policies, laws, and systems that change the structural conditions—such as access to transportation and health care—that influence and impact health outcomes. Political determinants of health can exist both at the formal level, seen in federal and local laws, and at the organizational level, through internal policies.
Poor mental health outcomes include a broad range of negative consequences resulting from undertreated or untreated mental health conditions, such as social isolation, impaired cognitive function, development of or worsening physical health conditions, and increased susceptibility to substance use. The root causes of poor mental health outcomes can be influenced by a multitude of factors spanning social drivers and political determinants of health, which collectively impact one’s overall health and well-being.31
Appendix 2: Data, data gaps, and exclusions
Varying reporting requirements: Information on the populations examined is not available from all data sources and measures used in this analysis. In addition, where they are reported, definitions of measures and populations may vary based on data sources.
Systemic barriers: Disaggregating health data by race and ethnicity poses challenges due to historical underreporting, misclassification, and privacy concerns. Without accurate data, identifying and addressing health inequities accurately becomes difficult, hindering progress toward achieving health equity and leaving marginalized communities underserved and overlooked in policymaking and resource allocation.
Cultural stigma: Cultural stigma continues to exist, particularly in minority groups, limiting self-reporting and willingness to seek care for mental health challenges.
Inequitable access to care: Due to inadequate mental health care access, not all population groups have the same likelihood of being diagnosed if they do have a mental health condition. Often federal- and state-funded community behavioral health centers are not located in the areas with the highest need of health care services.32 Addressing this issue may represent an opportunity to impact the inequitable outcomes experienced by marginalized groups. According to the Substance Abuse and Mental Health Services Administration’s research, there is a correlation between geographies lacking adequate access to mental health treatment resources and urban neighborhoods with a high level of racialized economic segregation and inadequate mental health resources.33
Uninsured population data: The primary analysis leverages data from Komodo Health, which is an extensive repository of claims data, with additional consultation of data from Medical Expenditure Panel Survey. The projections largely exclude populations who pay for their own health services due to being uninsured or underinsured. Therefore, the analysis is tilted toward the insured population, and the projected costs, while considerable, may in fact be conservative.
The School of Global Health at Meharry Medical College
The School of Global Health at Meharry Medical College exists to advance the well-being of the global community by establishing itself as a distinguished institution that educates and nurtures a diverse and inclusive cohort of passionate health leaders who can navigate political systems and societal structures to positively impact the public’s health. Building on the nearly 150 years of service and excellence by Meharry Medical College, the vision of the School of Global Health is to make health inequities history with a mission to empower leaders to catalyze solutions for the world’s most pressing and complex health challenges.
The Deloitte Health Equity Institute
The mission of the Deloitte Health Equity Institute is to advance health equity to make an impact that matters. To do it, we’re creating cross-sector collaborations and tools aimed at addressing disparities in the drivers of health, racism and bias, and structural flaws in the health system. Our goal is to create exponential change that will lead to a world in which health isn’t determined by race, gender, ability status, or zip code—one in which all people have the fair and just opportunity to achieve their full potential in every aspect of their health and well-being.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}