
Understanding physician network dynamics could help providers bring down health care costs Unlocking physician referral networks
11 minute read
29 January 2019



The focus on cost-efficiency under value-based care has health systems and providers looking to drive savings without sacrificing quality. Exploring the structure of physician networks may hold the key to one such opportunity.
Physicians are part of formal and informal networks in which they share patients, information, and clinical decisions. Deloitte’s analysis of these network dynamics in Medicare shows that where physician relationships are tightest, spending for certain health conditions is lower. For instance, an increase in physician centrality—a measure from network science that captures the degree of coordination between disparate parts of the network—decreases average episode-of-care cost for hip fracture by almost 15 percent (or US$2,000) and for coronary artery disease by 26 percent (or US$1,050). Our research shows that network concentration is especially important in larger networks, where having central physicians to help coordinate the flow of information/care is strongly associated with lower costs.
Learn More
View the interactive
Explore the Health care collection
Subscribe to receive related content from Deloitte Insights
The finding that these less-fragmented networks are in general more cost-efficient helps emphasize the importance of identifying key influencers within each community and prioritizing network design strategies (that is, creating high-performing networks for health plans and clinically integrated networks for health systems).
Health care organizations and health plans can consider mapping these relationships within their own geographic areas and patients/members. This can supplement conventional benchmarking approaches to understand opportunities for actively influencing care patterns and coordination among physicians with a view to improve financial and clinical performance.
Closer care coordination may be a key success factor in value-based care
Government, private payers, and employers are ramping up pressure on health systems, physicians, and other clinicians to not only improve quality, but also save money. Evaluations are showing early successes from investment in payment reform. For example, a recently released evaluation of the Pioneer ACO program found that this model saved more than US$384 million to Medicare over the last two years.1 However, performance under these programs varies: Many health systems have not generated savings in the Medicare Shared Savings Program. Many health systems and clinicians are looking for additional opportunities to drive savings without sacrificing quality.
MIPS and total cost-of-care measures
Under Medicare’s Merit-Based Incentive Payment System (MIPS) for physicians and other clinicians, payment is higher for clinicians with the highest scores for quality, quality improvement, and use of electronic health records and lowest scores for total cost of care. The measures of total cost of care attribute claims to specific clinicians based on their billing patterns; the costs include not only the services that the individual clinician billed, but all care within the episode (generally defined based on a condition and time-period).
For clinicians in the MIPS program, in 2019, cost measures will make up 15 percent of the total score; they rose from 0 in 2017 to 10 percent in 2018.2 For 2019, the cost-performance score will be based on performance in Medicare spending per beneficiary, total per capita cost, and episodes of care for particular health conditions.
With the cost measures, the challenge is performance, not reporting (since CMS does the calculation based on claims data). Clinicians and health systems will be paid more if they reduce costs while maintaining high levels of care quality. Understanding the care and utilization patterns of all the clinicians involved in the course of care will be essential for improving performance.
Analysis of naturally occurring practice patterns across primary care and specialist clinicians may point to opportunities for improving performance.
Previous analyses have shown that Medicare beneficiaries see a median of two primary care physicians and five specialists per year. Beneficiaries with certain chronic diseases see even more—a median of 8–10 physicians per year for heart failure and diabetes.3
It makes sense that network dynamics influence health care costs—that the closer the ties and communication among clinicians, the lower the costs. Long-standing research from John Wennberg and other researchers at Dartmouth has shown that health care costs are highest in areas with the largest supply of medical specialists.4 Moreover, an analysis of hospital-based professional networks based on patient-sharing ties found that physicians who have a greater number of connections have higher costs and more intensive care utilization.5
Indeed, some of the early successful payment reform experiments like the Alternative Quality Contract at Blue Cross Blue Shield of Massachusetts focused on technical assistance to clinicians on “analyses of condition-specific practice pattern variations [that] demonstrate how physicians within a given specialty—for example, cardiology—differ from their peers in their use of particular technologies, treatments, or diagnostic tests for patients with the same underlying clinical status.”6
Even though it is not the focus of this study, other researchers have found better quality outcomes with closer coordination among physicians, particularly when primary care physicians have a more central role.7
Medicare Advantage flexibility could build from insights about physician networks
CMS now allows Medicare Advantage plans the flexibility to improve value for members. For example, plans can now tailor benefits to members with particular health conditions under the value-based insurance design program (VBID) and Uniform Flexibility. They are also allowed to provide incentives for members to go to “high-value providers.” Network analysis could provide insight into which physicians and networks of physicians are best-positioned to participate in these programs.
Analysis shows physician centrality could help bring down cost of care
Physicians are part of formal and informal networks in which they share patients, information, and clinical decisions. Network analysis lets us measure the influence of each physician and how different characteristics of care patterns affect costs for certain conditions. We find that the tighter the relationships, regardless of the number of clinicians, the better the performance across all the episodes we studied.
Research methodology
We focused on six conditions that physician experts identified as having care and treatment patterns that are relatively predictable—cerebrovascular disease, chronic obstructive pulmonary disease, coronary artery disease, fracture/dislocation of the hip/femoral head, hypertension (essential), and spinal/back disorders, lower back.
We mapped the structure of physician networks providing care to patients with these conditions using 2015 Medicare fee-for-service claims for three states—Illinois, Massachusetts, and Florida. If physicians shared patients during an episode of care, we counted them as connected to each other for each condition and state. We grouped physicians in each network into “communities” of care using network detection algorithms and used regression analyses to measure the relationship between network characteristics and average spending per episode.
We also calculated physician centrality, a measure of the tendency of a physician to provide access to other physicians and facilitate the flow of information across disparate parts of the network. Visually, more central physicians tend to be positioned toward the middle, rather than the periphery, of a network (see Appendix 1).
We found that in general, physicians with more connections and physicians in higher-cost communities have higher costs of care. However, even after controlling for the number of connections and community affiliation, the tighter the shared-patient physician networks and the more central a physician is in a network, the lower the average costs of the episode. This holds true across the three states and all six conditions we studied, although the magnitude of the savings varied from a low of US$220 for lower back disorders to US$2,050 for hip fracture. We found that the more central physicians are within their “communities,” the greater the savings.
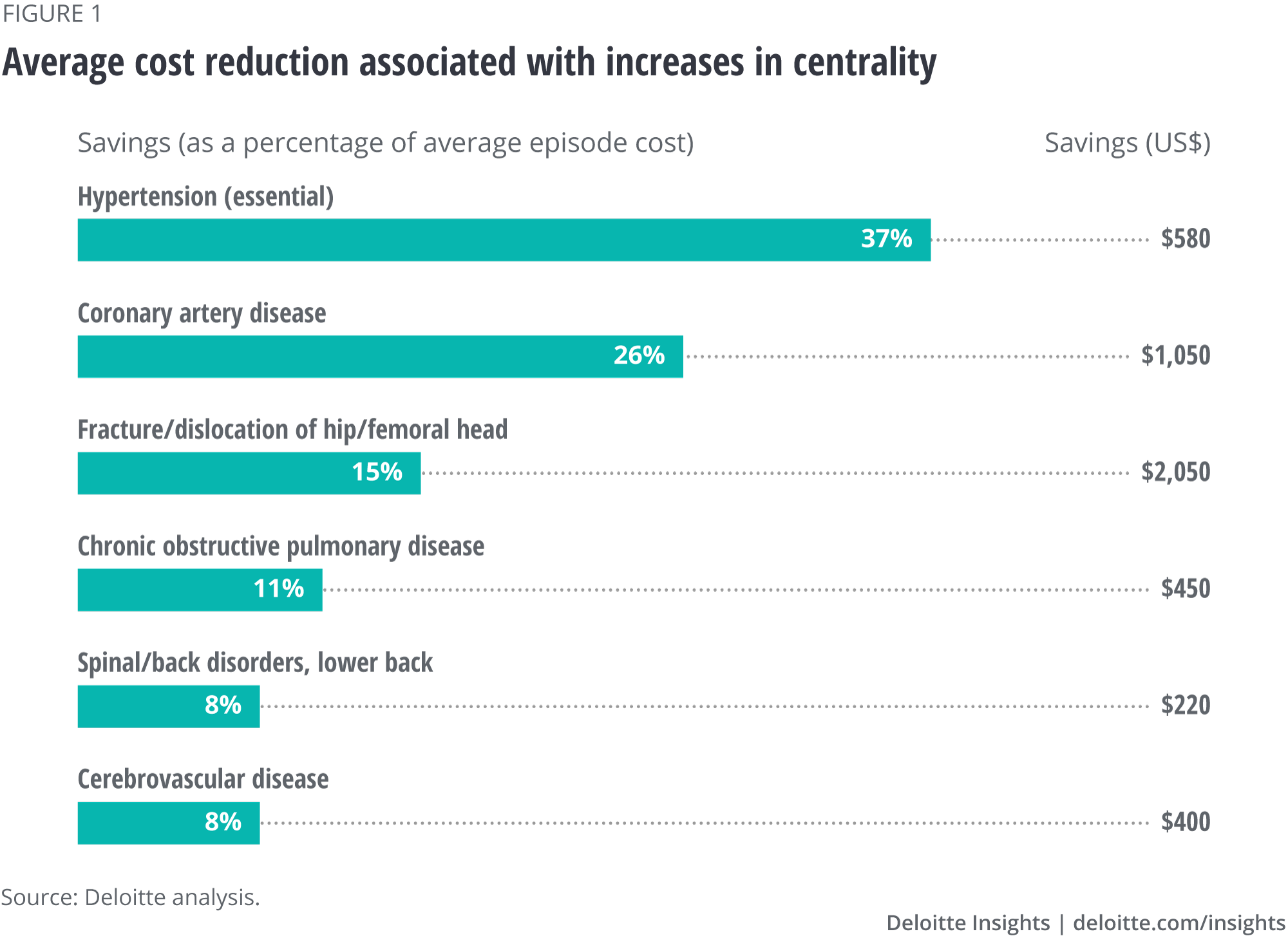
Tighter networks appear not only to reduce physician costs (see figure 1) but also certain nonphysician costs as well. In addition to savings in the cost of physician services, reductions in certain nonphysician components of episode costs—outpatient services, skilled nursing facilities, and ancillary services—generally account for a large share of savings in tighter networks for all the conditions that we studied, although the size of our data samples is smaller (see Appendix 1). These findings are consistent with physicians who are more “central” having lower episode costs by potentially managing information flows between separate parts of the network.
Explore the interactive below by using the filters and hovering over the boxes.
What health systems and plans can do with care pattern information
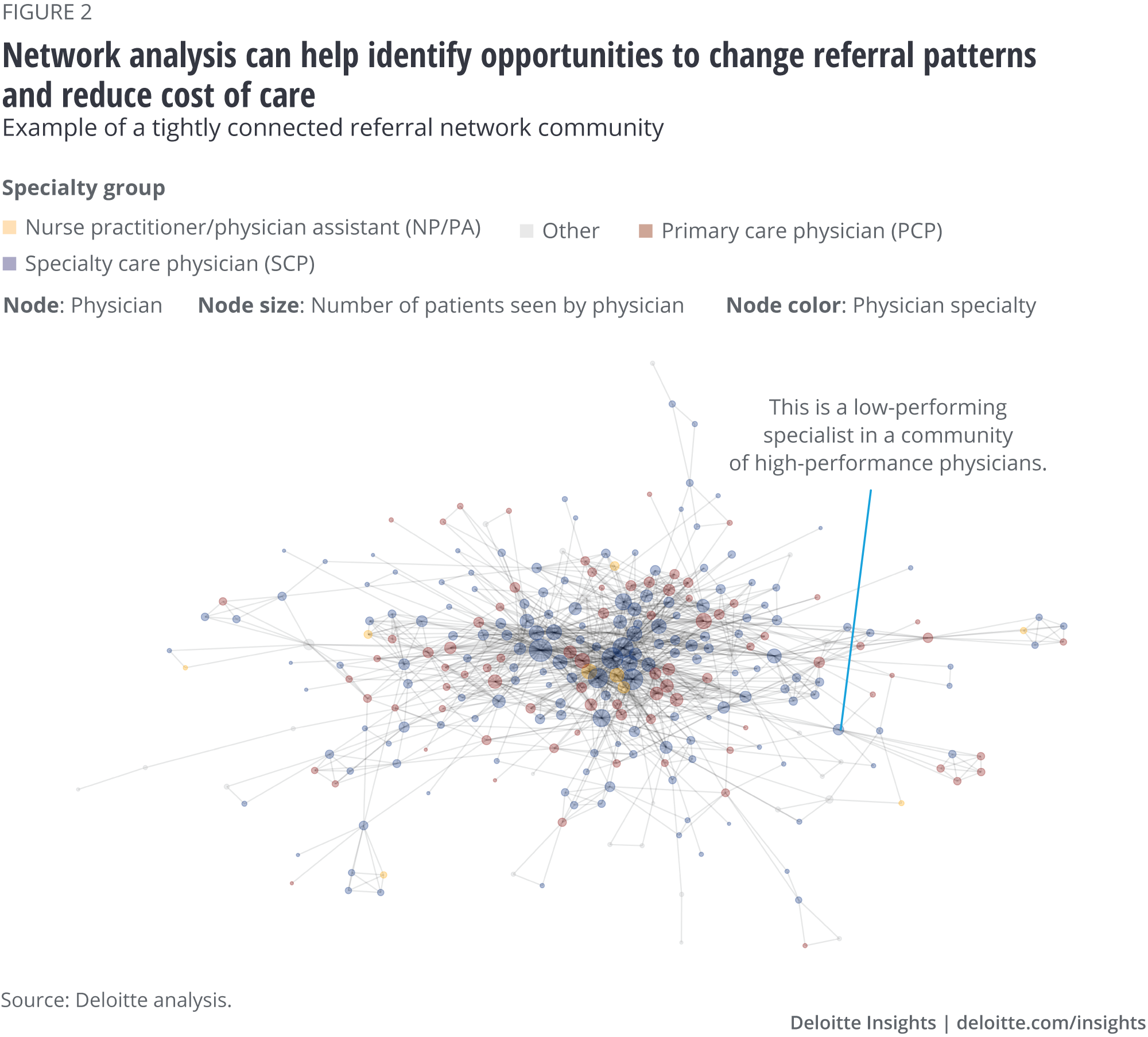
Both health systems and health plans have opportunities to improve their performance by better understanding and influencing care patterns, including referrals. Within each care network, a health system or a health plan can use claims data to identify high-performing and lower-performing networks and all the physicians who are part of the network. For example, in figure 2, one can find a specific cardiologist whose costs are higher compared to those of the other physicians in that cardiologist’s network. Health systems and plans could share this information with physicians and patients/members to encourage them to change their care patterns and referrals.
Health system perspective
From the health system perspective, the type of opportunity will likely depend on whether the organization is actively involved in new payment models that reward lower total cost of care or are largely paid under fee-for-service approaches that reward volume (see sidebar, “Health system opportunities”).
Health system opportunities
Fee-for-service. Under fee-for-service, which is still the more common of the two, opportunities are focused on increasing market share, which can be accomplished by referrals and volume. This is particularly important for facilities, as they have large fixed expenses. Understanding referral patterns can help organizations see where there are leakages of patients to nonnetwork clinicians and other providers, resulting in a loss of revenue opportunities. Physicians seeing Medicare patients in these types of health systems are, however, likely to see payment adjustments in the future based on total cost of care, as described earlier.
New payment models. For health systems with more payment at financial risk for total cost of care, the analysis would be similar, although how the analysis is applied would be different. In this case, organizations will likely want to consolidate services with the lower-cost physicians and share cost information with physicians to improve performance. The more efficient physicians likely use fewer facility services. So, another goal could be to get to lower medical expenses per member and associate themselves with a lower-premium insurance product (increasing market share) to fill excess facility capacity generated by more efficient physician performance.
Regardless of whether the goal is to increase volume, decrease the total cost of care, or improve quality, our experience has shown that the following steps can lead to better performance:
Empower a physician leader to be in charge of the initiative. Physicians tend to have more influence and credibility with other physicians.
Define and communicate the goals of the referral pattern analysis and dig deep into the reasons for the patterns; for example, why are referrals going outside of the network? Reasons for using out-of-network services can include long waits for appointments, long-standing habits and relationships, and services not being offered as part of the health system network. Sometimes the issue may lie not with the physician but with the office staff, who might prioritize routine and access if the physician does not name a particular referral resource.
Based on this research, pick the issues to work on where the system can garner “quick wins”; for example, meeting with practice leaders in specialties like orthopedics and cardiology and assuring referring physicians that their patients can get quicker appointments.
Continue to provide feedback and actionable information to referring physicians specific to their panel of patients and communicate the success of the initiative in meeting its goals to improve patient care and organizational performance. Setting reasonable goals and expectations for change that makes the difference can be another crucial part of this feedback.
Beyond referral information, share information with physicians on how they can improve their performance by providing them with data that shows how their patterns compare with network averages for diagnostic rate, hospital admission rate, surgery rate, and other measures.
Health plan perspective
From the health plan perspective, influencing referral patterns can help them meet their goals for reducing cost of care. Tools available range from product design to patient incentives, as well as the approaches available to health systems (especially relevant if the health plan is provider-sponsored or owns physician practices).
Health plans can use this information in two ways. One is targeting the right providers for high- performance networks and condition-specific bundled payment arrangements. Especially with the Medicare Advantage VBID and Uniform Flexibility programs, health plans are exploring how to combine benefit design and network levers to provide incentives that steer members to high-performing providers. The second way to use this information is through network analysis at the condition-specific level to identify primary care and specialty physicians to target for high-priority conditions with the most variation in care. Providing timely and actionable data to providers can help them reduce unwarranted variation; that is, show physicians how they compare with the best-performing providers within the same network—the key influencers—and what they can do differently to optimize performance.
Classic approaches to managing referral patterns and keeping the network tight are in the traditional health maintenance organization model, which typically has a narrower network of physicians and may require patients to get a referral from primary care clinicians to see a specialist. These models are seeing something of a resurgence in popularity in both Medicare Advantage and health exchanges. Even in preferred provider organization models, the health plan can use analyses of care and referral patterns to decide which clinicians to include as preferred or as participating clinicians. Utilization management strategies also can limit referrals for particular procedures or types of services.
New technologies are becoming available to support physicians in deciding whether a referral is even necessary. The Community eConsult Network, for example, uses teleconsults to support the primary care referrer virtually. A peer-reviewed study found that this service “improved access to and timeliness of care for an underserved population, reduced overall specialty utilization, and streamlined specialty referrals without any increase in adverse cardiovascular outcomes.”8
Organizations are using strategies and technologies to help members reduce redundant care (and potentially avoid the need for referrals) through dedicated call centers. Companies like Accolade and Quantum have been offering this service to self-insured employers to help members understand their benefits, remind them of preventive care, and advise them on whether they need services like imaging if they have already had a recent image for another clinician.
APPENDIX 1: Data and model
We used the 2015 5 percent Limited Data Set Medicare claims data for Florida, Illinois, and Massachusetts to “map” the structure of physician referral networks for six conditions that Deloitte physician experts recommended as having care and treatment patterns that are relatively predictable: cerebrovascular disease, chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD), fracture/dislocation of the hip/femoral head, hypertension (essential), and spinal/back disorders, lower back.9 Episodes of care were identified using the Truven Health Medical Episode Grouper.
We modeled the relationship between physicians as a one-mode projected bipartite undirected network with simple weighting, where the nodes are physicians and edges/ties arise from patients shared during an episode of care.10 Separate networks were constructed for each condition and state. Episode-level analysis helps exclude potentially spurious linkages between physicians treating common patients for unrelated reasons. Episodes of care that resulted in the death of a patient and those where the majority of services were performed by physicians who reside out-of-state were excluded from the analyses.
We grouped physicians into “communities” by applying a community-detection algorithm—the fast greedy modularity optimization algorithm—commonly used in large-scale networks.11 Communities are defined as groups of nodes (physicians) that are more densely connected to one another than to other nodes.12
Using these networks and communities, we performed regression analyses to assess whether a key network characteristic—centrality—is associated with physician cost performance. In our baseline model, the dependent variable is the physician-level average episode cost of care (in log form). Our baseline network metric is centrality (normalized betweenness, which is defined below)—see Appendix 2. We also include controls for:
- The number of connections of a given physician (logarithm of the normalized degree)
- Number of episodes (indicators for medium, high, and very high number of episodes)
- Physician specialty (indicators for whether a physician is a primary care physician or specialist)
- Episode severity (indicators for whether a physician’s share of moderately and respectively highly severe episodes were above the median)
- Community affiliation (indicators for physician communities)
We also ran models where we analyzed the association between network centrality and six different components of average physician cost: inpatient, outpatient, physician, laboratory, skilled nursing facility, and ancillary costs. The direction of the association between centrality and these cost components was generally maintained, but the small sub-samples were not conducive to a deeper exploration of the mechanisms at play.
Appendix 2: Centrality measures

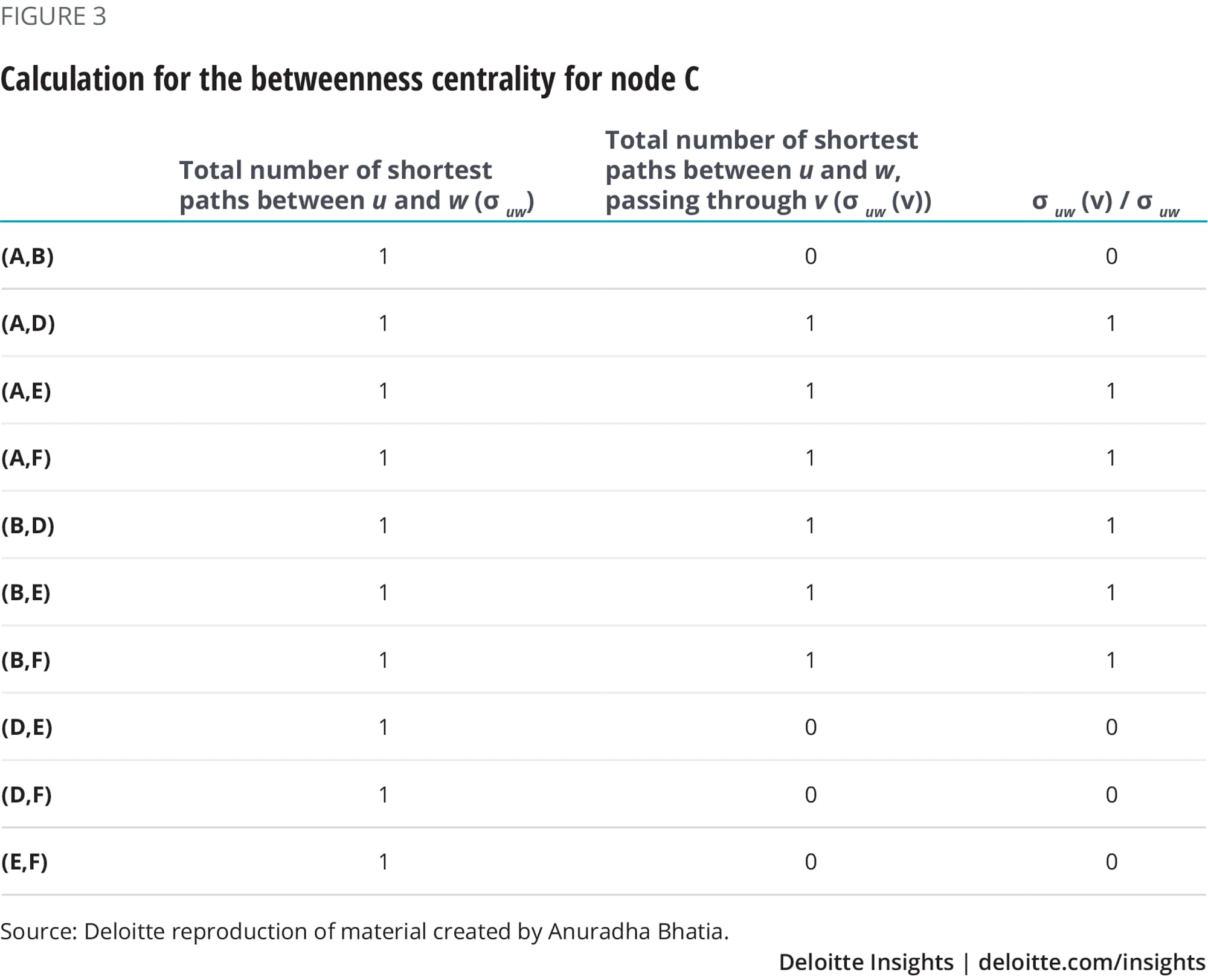
In our model, we define centrality using a commonly used metric in network science known as betweenness centrality. Betweenness is a measure of influence of a node over the flow of information in the network and it measures the number of shortest paths that pass through that node.13 Betweenness is important not only to achieve a more effective flow of information but also to connect different parts of the network. More formally, it is defined as shown to the left.
Figure 3 shows the calculations for Node C. Hence, betweenness centrality for node C=6. Similarly, we calculate the score for other nodes. A, B, E, and F = 0; D = 6. We can say that both C and D have high betweenness centrality. Nodes with high betweenness centrality are important controllers of the flow of information across the network.
We also performed robustness checks where we used a different operationalization of our centrality metric, namely page rank. The page rank score measures how important a node is in a given network, including where communities of isolated nodes may exist. Page rank looks at the number of connections that the node has to other nodes within the network while also taking into consideration the connections of those nodes.14
Deloitte Digital’s provider accelerator—Care Connect: connecting patients to care
Managing health care has changed. To be competitive today, health care providers need to address the major changes that are driving patient behavior and adopt a customer-service mindset. This emerging demand for customer-centric care is driving innovation and transforming the patient-centered experience—from appointment scheduling to timely access to billing information and transparency in health care purchasing decisions. Deloitte has drawn from its industry knowledge to identify areas of development associated with patient engagement, and uses leading practices to provide a sleek, solid foundation that can be customized to specific providers. Deloitte Digital's Care Connect accelerator can make patient-centered care a reality by providing a full-service solution to digital patient engagement.
Learn more
Get in touch

- James Whisler
- Principal
- Deloitte Consulting LLP
- jwhisler@deloitte.com
- +1 612 397 4045
Related content

Read more about health care
-
 Health care Collection
Health care Collection -
 Surveys of health care consumers and physicians Collection6 years ago
Surveys of health care consumers and physicians Collection6 years ago -
 Physicians are willing to manage cost but lack data and tools Article5 years ago
Physicians are willing to manage cost but lack data and tools Article5 years ago -
What can health systems do to encourage physicians to embrace virtual care? Article6 years ago
-
 Social determinants of health and Medicaid payments Article5 years ago
Social determinants of health and Medicaid payments Article5 years ago






