Sara Heath, “ACP calls to end health disparities, racial bias in healthcare,” PatientEngagementHIT, January 13, 2021.
View in ArticleCenters for Disease Control and Prevention, Risk for COVID-19 infection, hospitalization, and death by race/ethnicity, March 25, 2022.
View in ArticleWilliam F. Marshall, “Coronavirus infection by race: What's behind the health disparities?,” Mayo Clinic, August 13, 2020.
View in ArticleHeath, “ACP calls to end health disparities, racial bias in healthcare.”
View in ArticleAmerican Medical Association, “AMA adopts guidelines that confront systemic racism in medicine,” press release, June 15, 2021.
View in ArticleJoe Sammen et al., Race is a social construct, Center for Health Progress, October 24, 2017.
View in ArticleCenters for Disease Control and Prevention, Data & statistics on sickle cell disease, March 30, 2022.
View in ArticleWGBH Educational Foundation and Clear Blue Sky Productions, “A mutation story,” video, 2001.
View in ArticleCenters for Disease Control and Prevention, Data & statistics on sickle cell disease; ASH Foundation, ASH Sickle Cell Disease Initiative Fund, 2022.
View in ArticleAmerican Academy of Family Physicians, “Race based medicine,” July 2020.
View in ArticleTimothy M. Smith, “Race-based medicine is wrong. How should physicians oppose it?,” American Medical Association, December 14, 2020.
View in ArticleAmerican Medical Association, “New AMA policies recognize race as a social, not biological, construct,” press release, November 16, 2021.
View in ArticleJohn P. A. Ioannidis, “Recalibrating the use of race in medical research,” Jama Network, January 25, 2021.
View in ArticleCara V. James et al., “Modernizing race and ethnicity data in our Federal Health Programs,” The Commonwealth Fund, October 26, 2021.
View in ArticleCenters for Disease Control and Prevention, “Demographic characteristics of people receiving COVID-19 vaccinations in the United States,” 2022.
View in ArticleAlexander Ladenheim, “Race and eGFR: Addressing health disparities in chronic kidney disease,” UC Davis Health, April 29, 2021.
View in ArticleTheresa Gaffney, “A yearslong push to remove racist bias from kidney testing gains new ground,” STAT, July 17, 2020.
View in ArticleJames A. Diao, Gloria J. Wu and Herman A. Taylor, “Clinical implications of removing race from estimates of kidney function,” no. 2, pp. 184-186.
View in ArticleThe New England Journal of Medicine, “Racial bias in pulse oximetry measurement,” December 17, 2020.
View in ArticleZachary Vesoulis et al., “Racial discrepancy in pulse oximeter accuracy in preterm infants,” Journal of Perinatology, (2022): pp. 79–85.
View in ArticleDavid R. Roediger, “Historical foundations of race,” National Museum of African American History & Culture, accessed April 25,2022.
View in ArticleStaffan Muller-Wille, "Race and History: Comments from an Epistemological Point of View," Sci Technol Human Values (2015): pp. 597-606.
View in ArticleRaj Bhopal, "The beautiful skull and Blumebach's errors: the birth of the scientific concept of race," BMJ (2007): pp. 1308-9.
View in ArticleFacing History & Ourselves, "The Science of Race: Holocaust and Human Behavior," accessed May 9, 2022.
View in ArticlePaul Wolff Mitchell, "The fault in his seeds: Lost notes to the case of bias in Samuel George Morton's cranial race science," PLoS Biol (2018).
View in ArticleAyah Nuriddin, Graham Mooney, and Alexandre I R White, “Reckoning with histories of medical racism and violence in the USA,” Elsevier Public Health Emergency Collection, (2020): pp.949–951.
View in ArticleMeredith A Anderson, Atul Malhotra and Amy L Non, “Could routine race-adjustment of spirometers exacerbate racial disparities in COVID-19 recovery?,” The Lancet Respiratory Medicine, no. 2(2021): pp. 124-125.
View in ArticleCenters for Disease Control and Prevention, “About the National Health and Nutrition Examination Survey,” accessed April 25,2022.
View in ArticleMeredith A Anderson, Atul Malhotra and Amy L Non, “Could routine race-adjustment of spirometers exacerbate racial disparities in COVID-19 recovery?”
View in ArticleAmerican Thoracic Society, “Removal of “race correction” in pulmonary function tests shows more prevalent and severe lung disease among black patients,” press release, May 16, 2021.
View in ArticleMegan Gannon, “Race is a social construct, Scientists argue,” Scientific American, February 5, 2016.
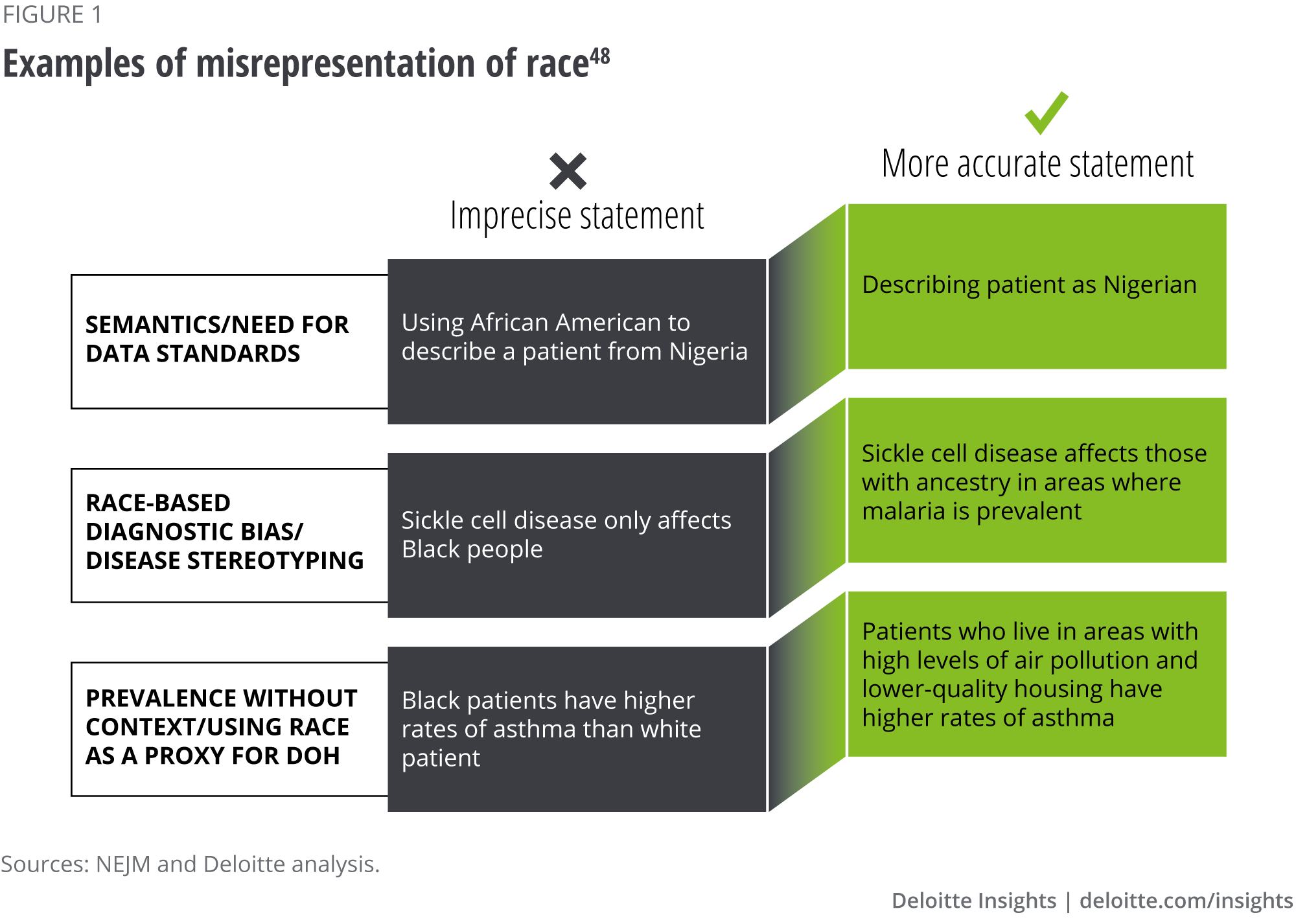
View in ArticleChristina Amutah et al., “Misrepresenting race — The role of medical schools in propagating physician bias,” The New England Journal of Medicine, March 4, 2021.
View in Article-
NewYork-Presbyterian, “Dalio Center for Health Justice,” accessed April 25, 2022; Northwell Health, “We ask because we care,” accessed April 25, 2022; Stanford Medicine, “Health Equity—Our mission,” accessed April 25, 2022.
View in Article
Agency for Healthcare Research and Quality, Defining categorization needs for race and ethnicity data, accessed April 25, 2022.
View in ArticleMartha Hostetter, “Confronting racism in health care,” The Commonwealth Fund, October 18, 2021.
View in ArticleAmutah et al., “Misrepresenting race — The role of medical schools in propagating physician bias."
View in ArticleMichelle Tong and Samantha Artiga, “Use of race in clinical diagnosis and decision making: Overview and implications,” Kaiser Family Foundation, December 9, 2021.
View in ArticleNEJM roundtable
View in ArticleAna Sandoiu, “'Weathering': What are the health effects of stress and discrimination?,” Medical News Today, February 26, 2021.
View in ArticleRachel Nuzum, Corinne Lewis and Debbie I. Chang, “Measuring what matters: Social drivers of health,” The Commonwealth Fund, November 6, 2021.
View in ArticleAlexander Billioux et al., “Standardized screening for health-related social needs in clinical settings: The accountable health communities screening tool,” National Academy of Medicine, May 30, 2017.
View in ArticleMaani Kamal, “Episode 141: Antiracism in medicine series episode 2 – Dismantling race-based medicine part 1: Historical and ethical perspectives with Edwin Lindo,” November 17, 2020.
View in ArticleSusan G. Komen, “Breast Cancer Risk: Race and ethnicity,” March 15, 2022.
View in ArticleACS Medical Content and News Staff, “More black women die from breast cancer than any other cancer,” American Cancer Society, February 14, 2022.
View in ArticleValentina A. Zavala et al., “Cancer health disparities in racial/ethnic minorities in the United States,” British Jornal of Cancer, (2021): pp. 315-332.
View in ArticleKomen, “Breast Cancer Risk.”
View in ArticleAmutah et al., “Misrepresenting race — The role of medical schools in propagating physician bias."
View in ArticleMichael W. Kattan, “Clinical algorithms, encyclopedia of medical decision making,” accessed April 25, 2022.
View in ArticleCarmi Z. Margolis, “Uses of clinical algorithms,” Jama Network, February 4, 1983; Andis Robeznieks, “Feds warned that algorithms can introduce bias to clinical decisions,” American Medical Association, June 23, 2021.
View in ArticleSharon Begley, “Racial bias skews algorithms widely used to guide care from heart surgery to birth, study finds,” STAT, June 17, 2020.
View in ArticleDarshali A. Vyas, Leo G. Eisenstein, and David S. Jones, “Hidden in plain sight — Reconsidering the use of race correction in clinical algorithms,” The New England Journal of Medicine, August 27, 2020.
View in ArticleBegley, “Racial bias skews algorithms widely used to guide care from heart surgery to birth, study finds.”
View in ArticleVyas, Eisenstein, and Jones, “Hidden in plain sight,” The New England Journal of Medicine.
View in ArticleIbid.
View in ArticleIbid.
View in ArticleUnderstanding African American and non-African American eGFR laboratory results | National Kidney Foundation
View in ArticleAgency for Healthcare Research and Quality, Impact of healthcare algorithms on racial and ethnic disparities in health and healthcare, January 25, 2022.
View in ArticleLadenheim, “Race and eGFR: Addressing health disparities in chronic kidney disease,” UC Davis Health; A S Levey et al., “A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of diet in renal disease study group,” National Library of Medicine, March 16, 1999.
View in ArticleAgency for Healthcare Research and Quality, Impact of healthcare algorithms on racial and ethnic disparities in health and healthcare.
View in ArticleVyas, Eisenstein, and Jones, “Hidden in plain sight,” The New England Journal of Medicine.
View in ArticleJonathan Greig, “NYC creates coalition to end bias and 'race norming' in medical algorithms,” ZDNet, December 13, 2021.
View in ArticleCynthia Delgado et al., “A Unifying Approach for GFR Estimation: Recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease,” American Journal of Kidney Disease, no.2 (2022): pp. 268-288
View in ArticleAnuja Vaidya, “NYC Health + Hospitals drops use of two race-based clinical assessments,” MedCityNews, May 18, 2021.
View in ArticleElise G. Valdes, “Examining cesarean delivery rates by race: a population-based analysis using the robson ten-group classification system,” Journal of Racial and Ethnic Health Disparities, (2021): PP. 844-851.
View in ArticleMayo Clinic, “Vaginal birth after cesarean (VBAC),” June 09, 2020.
View in ArticleKatie Palmer, “Changing the equation: Researchers remove race from a calculator for childbirth,” STAT, June 3, 2021.
View in ArticleVyas, Eisenstein, and Jones, “Hidden in plain sight,” The New England Journal of Medicine.
View in ArticleElise G. Valdes, “Examining cesarean delivery rates by race: a population-based analysis using the robson ten-group classification system."
View in ArticleCenter for Applied AI at Chicago Booth, Algorithmic bias playbook, 2021.
View in ArticleZiad Obermeyer, “Dissecting racial bias in an algorithm used to manage the health of populations,” Science, October 25, 2019.
View in ArticleMichael Roberts et al., “Common pitfalls and recommendations for using machine learning to detect and prognosticate for COVID-19 using chest radiographs and CT scans,” Nature Machine Intelligence, March 15, 2021.
View in ArticleUC AI Working Group Final Report (ucop.edu)---------------------- Link not working. Please ask the author to send the correct/alternative link
View in ArticleIbid.
View in ArticleUS Food & Drugs Administration, Artificial Intelligence/Machine Learning (AI/ML)-Based software as a Medical Device (SaMD) Action Plan, January 2021.
View in ArticleUS Food & Drugs Administration, “Good machine learning practice for medical device development: Guiding principles,” October 27, 2021.
View in ArticleBolajoko O. Olusanya et al., "Transcutaneous bilirubin nomograms in African neonates," PLoS One (2016).
View in ArticleSubcommittee on Hyperbilirubinemia, "Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation," Pediatrics (2004): 297-316.
View in ArticleAmerican Academy of Pediatrics, "American Academy of Pediatrics Calls for Elimination of Race-Based Medicine," May 2, 2022.
View in ArticleMichelle Tong and Samantha Artiga, “Use of race in clinical diagnosis and decision making: Overview and implications,” KFF, December 9, 2021.
View in ArticleWhitney J. Palmer, “Black women twice as likely to experience breast cancer diagnostic delay,” Diagnostic Imaging, July 20, 2021.
View in ArticleLinda Goler Blount, “Black women are receiving inferior breast screening,” Imaging Technology News, July 6, 2021; Maria Aspan, “‘We can’t ever go to the doctor with our guard down’: Why Black women are 40% more likely to die of breast cancer,” Fortune, June 30, 2020.
View in ArticleErin Brodwin and Nicholas Fleur, “‘These numbers are incredibly important’: Doctors and lawmakers call on FDA to address racial disparities in pulse oximeters,” STAT news, February 10, 2021; Tori Rodriguez, “Pulse oximetry: Examining racial bias in a valuable but flawed tool,” Pulmonology Advisor, April 2, 2021.
View in ArticleTiffany L. Green et al., “Rethinking bias to achieve maternal health equity: Changing organizations, not just individuals,” Obstetrics and Gynecology 137, no. 5 (2021): pp. 935–40.
View in ArticleJamila Taylor et al., Eliminating racial disparities in maternal and infant mortality, Center for American Progress, May 2019.
View in ArticleRutgers University, “African-Americans more likely to be misdiagnosed with schizophrenia,” ScienceDaily, March 21, 2019.
View in ArticleJune Liang, Brittany E. Matheson, and Jennifer M. Douglas, “Mental health diagnostic considerations in racial/ ethnic minority youth,” Journal of Child and Family Studies 25, no. 6 (2016): pp. 1, 926–40; Mental Health America, “Black and African American communities and mental health,” accessed March 16, 2022; Tahmi Perzichilli, “The historical roots of racial disparities in the mental health system,” Counseling Today, May 7, 2020.
View in ArticleChristina Caron, “Why are more Black kids suicidal? A search for answers,” New York Times, November 18, 2021.
View in ArticleMonika K. Goyal et al., “Racial disparities in pain management of children with appendicitis in emergency departments,” JAMA Pediatrics 169, no. 11 (2015): pp. 996–1002.
View in ArticleDarshali A Vyas, Leo G. Eisenstein, and David S. Jones, "Hidden in Plain Sight--Reconsidering the Use of Race Correction in Clinical Algorithms," New England Journal of Medicine 383(2020): 874-882.
View in ArticleEnrique Rivero, “Black patients’ Lyme disease often diagnosed late, possibly due to missed signs,” UCLA Newsroom, September 30, 2021.
View in ArticleJanice A. Sabin, “How we fail black patients in pain,” AAMC, January 6, 2020.
View in Article















{kind=link}
{kind=link}