Broadening research participation through community engagement
Community Health Centers can help increase the diversity and scope of clinical studies—and ultimately, improve patient outcomes.


Dawn Anderson

Jessica Nadler

Julia Skapik

Amy Flowers

Christine Chang

Jessica Overman
Systemic change is needed across the US clinical research system to address the lack of diversity among research participants.1 This effort will require finding new partners. Bringing in new voices. Implementing new policies. Investing in new infrastructure. Providing new incentives. Inventing new business models. And pursuing new research approaches. Moreover, trust must be rebuilt between traditional research institutions and communities.
Community Health Centers, which already serve as an essential component of the health care landscape, play a critical role in advancing more equitable and inclusive research.2 Given their footprint in the community, patient-centered, trusted relationships, and diverse patient populations,3 health centers can enrich the diversity and scope of clinical studies and, ultimately, enhance patient outcomes.
However, health centers are often not approached or seen as key partners in the clinical research ecosystem. They have also been wary of participating due to historical ethical concerns and an ongoing lack of transparency (for example, the US Public Health Service Syphilis Study at Tuskegee, among others).4 Another barrier is the lack of funding and clinical research infrastructure that inhibits those interested in conducting research from identifying and pursuing clinical research opportunities.
To highlight the critical role that health centers play in advancing more equitable and inclusive research5 and identify the resources and support needed to conduct and sustain these efforts, the National Association of Community Health Centers (NACHC) and the Deloitte Center for Health Solutions collaborated on a survey of 226 health center chief executive officers (or their designees) between May and June 2023. The Deloitte Center for Health Solutions also conducted 22 interviews with a wide range of research stakeholders, including research and clinical leaders from health centers, academic institutions, and research organizations, between July and October 2023 to gain additional insight into research processes and collaborations.
Through the survey and interviews, we explored key questions like, what can be learned from health centers that are already conducting research? How can health centers that are interested in pursuing research get started? And what entities could they potentially partner with on research? As one chief innovation and strategy officer we interviewed stated, “Health centers are trusted and can be the intermediary to build trust in communities that have been historically kept out of the research process and taken advantage of. But then the question is ‘how.’”
What are Community Health Centers?
Community Health Centers, also known as health centers, federally qualified health centers (FQHCs), or FQHC look-alikes, provide comprehensive primary care services to medically underserved areas and populations.6 In 2022, health centers cared for 31.5 million patients (which is roughly one out of every 11 Americans). The communities they serve are diverse in a myriad of ways: 19% of health center patients are uninsured, 61% are publicly insured, 90% are low-income, 41% are rural, and 64% are members of racial and/or ethnic minority groups.7 While each health center may have specific priorities for their communities, generally, health centers have patients with higher rates of hypertension, high cholesterol, asthma, and diabetes than the general population, all of which could be natural areas of research interest.8
Diverse representation in research, particularly clinical trials is critical for building trust in medical research and institutions, promoting fairness for potential participants and their community, and generating biomedical knowledge of treatment efficacy for all patients.9 Yet, clinical research is generally not inclusive of racial and ethnic minority groups, as well as other populations experiencing health disparities, including sexual and gender minorities or socially disadvantaged populations.
Excluding historically marginalized populations from participating in research poses a threat to health equity and can exacerbate existing disparities, which cost about $320 billion per year.10 As one of the health policy research directors we interviewed said, “Health centers and their patients have an important story to tell. They can make an important contribution to health equity.”
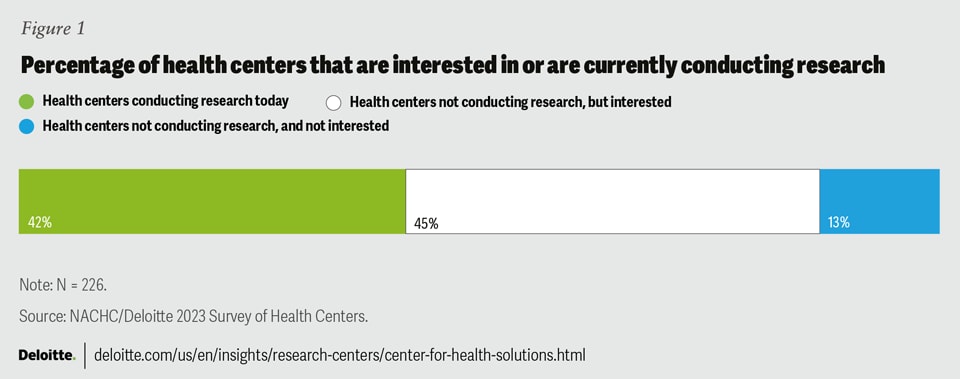
Most health centers are interested in conducting research
We found that 87% of health centers are either currently conducting research or are interested in conducting research. Forty-two percent of surveyed respondents are already conducting research today and 45% are interested in conducting research (figure 1).

According to the surveyed health centers currently engaged in research, health services research11 is the most prevalent type, undertaken by 54% of these centers. Additionally, 36% of these survey respondents are conducting participatory action research.12 Many of the interviewees highlighted the significance of participatory action research in empowering community members to actively engage in research, which then results in more impactful and meaningful research outcomes.
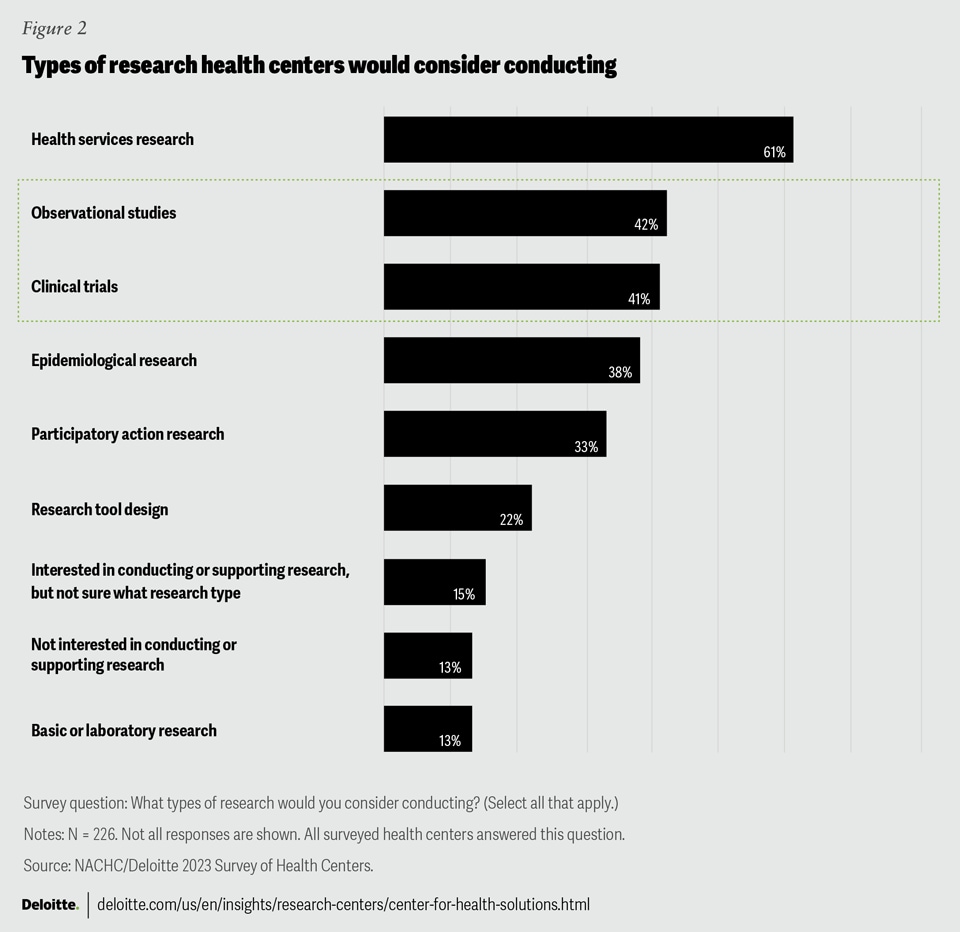
Health centers are interested in clinical research, a category that encompasses both clinical trials and observational studies, as well (see figure 2). Among the surveyed health centers currently engaged in research, 53% are actively involved in clinical research, with 37% conducting observational studies and 34% conducting clinical trials.13 Health centers in urban areas are significantly more inclined to conduct clinical trials (21%), compared with just 4% of health centers located in rural areas. Furthermore, among health centers interested in but not currently conducting research, 44% are interested in conducting clinical research, including clinical trials (35%) and observational studies (32%).

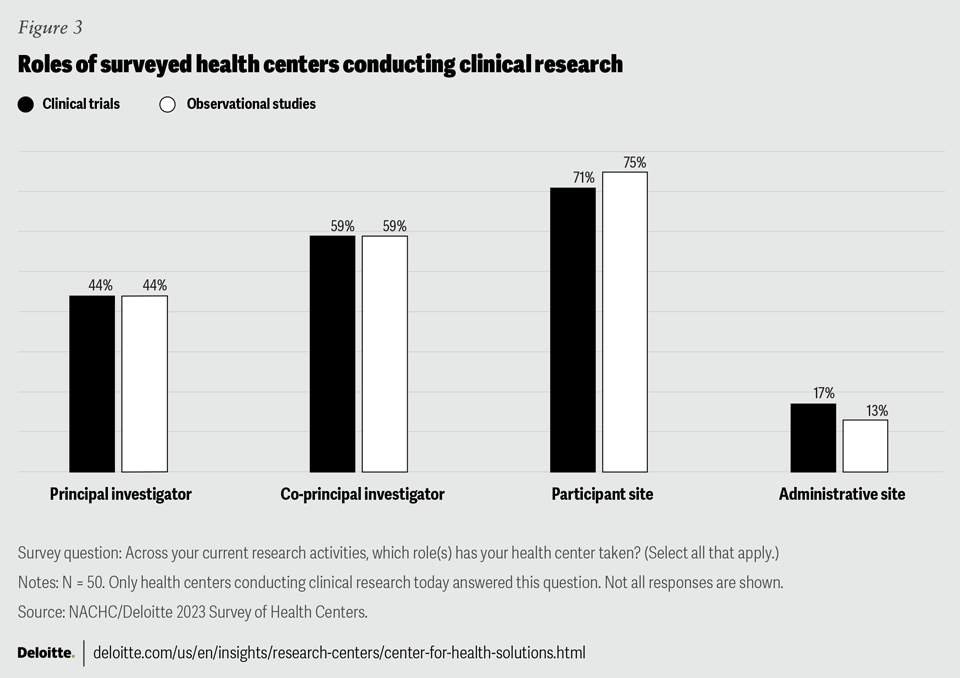
Most surveyed health centers that conducted clinical research served as participant sites and acted as co-principal investigators (figure 3). Surveyed health centers that serve predominately white patients are more than twice as likely to act as the principal investigator for a study compared to those that serve predominately Black (18%) and Hispanic (14%) patients. Additionally, those in urban areas are much more likely to act as the principal investigator (24%), co-principal investigator (24%), or participant site (32%) compared to those in rural settings (4%, 11%, and 11% respectively).
Most interviewees expressed interest in leading the research instead of supplying data to a research partner. Taking a leading role can enable health centers to focus on research that directly benefits their patients and provides their staff with new skills.

Benefits to conducting research: Improved community health outcomes
Surveyed health centers that are currently working on research and interested in research cited improved community health outcomes and engagement as the most beneficial aspect of research to the organization. For surveyed respondents who are not currently conducting research but are interested, increased funding opportunities/revenue streams were the top perceived benefit of conducting research.
Workforce development and professional growth was the second highest rated benefit to health centers that conduct and are interested in research. Many interviewees remarked how, particularly in the current health care workforce environment, providing additional types of work and training has helped retain staff. One interviewed participant cited, “It is a competitive advantage to enable the workforce to conduct research.” For another interviewee, participating in research plays a significant role in enhancing the reputation and visibility of the health center.
As a survey respondent wrote, “We believe that our organization and our patients benefit greatly from participating in research ... By housing research within a community facing organization and allowing our staff in partnership with our patients and providers to decide what is relevant to OUR communities and how we want to engage with research (and evaluation), it has opened the door to better understanding, better participation and ultimately, better health outcomes for our patients. We need to do research not for research’s sake, but for the short- and long-term benefit of our patients.”
Barriers to participation: Time and workforce constraints
The barriers to participating in research are generally well-known but can vary from health center to health center depending on the community that they serve. They are not, however, insurmountable. Eighty-one percent of survey respondents do not have dedicated staff to perform research and 88% do not have budget/resources dedicated to conducting research. Not surprisingly, the biggest barriers for survey respondents conducting and/or interested in research were time or workforce constraints (94%) and funding (81%).
Research expertise is a top challenge for 61% of health centers located in rural areas versus just 39% of health centers in urban areas. Health centers that serve predominately Black patients are more than twice as likely to cite challenges with retaining patients as a top challenge for conducting or supporting research (23%), compared to those that serve predominately white patients (10%).
For the 13% of survey respondents who were not interested in research, the top reasons were that it was too burdensome (for example, lack of time) (77%), insufficient funds (67%), and lack of research expertise (57%). Just 7% of respondents didn’t see any value in conducting research. These survey respondents noted that greater research expertise and funding could encourage them to participate in research.
81% of survey respondents do not have dedicated staff to perform research and 88% do not have budget/resources dedicated to conducting research.
As one interviewee noted, research is often considered a “luxury” at health centers. Another interviewee preferred to refer to research as quality improvement, which can allay some of the patient trust issues but may limit the types of research that a health center would focus on. Despite these obstacles, some health centers have found ways to fund and sustain the resources needed to do research (see sidebar, “Erie Family Health Centers set up a research governance process,” for more information).
Infrastructure is needed to expand research capacity
Interviewees shared their experiences of how research began at their health centers, often driven by a curious clinician dedicating extra hours after work or on weekends. When initial findings emerged, securing funding or protected research time became possible. Occasionally, collaboration opportunities arose when potential research partners approached them. Enhanced research infrastructure can empower health centers to pursue research endeavors proactively and systematically.
Health centers require diverse and extensive infrastructure support to facilitate research. This encompasses physical spaces for participant interactions, research training and skills development, as well as dedicated time. All of which can be addressed through increased funding. Additionally, essential infrastructure elements include leadership interest and support, streamlined governance procedures, access to Institute Review Boards (IRBs), and specific technology requirements.
Governance processes and leadership support
Research activities are overseen by different roles at each health center. Nearly 50% of survey respondents currently conducting research stated that the chief medical officer oversees research at their centers, but that chief executive officers, chief quality officers, research leads, population health departments, chief operating officers, and others were also involved in the process.
Interviewees felt strongly that gaining leadership interest and support was necessary to sustain research efforts. However, one interviewee stated that there is a perception among some C-suite leaders who are less inclined to support research that the main outcome in conducting research is to publish papers, but “publishing papers is not a primary goal or driver of research; rather it is to make an impact.” While patient care would always come first, interviewees noted that research can support many other health center goals including advocacy, policy, and quality improvement.
Several interviewed health centers also cited that they do not have their own IRB, which is necessary to conduct clinical research. Often, they use IRBs through partnerships with academic medical centers. They also can hire a commercial or private IRB, however, a few interviewees expressed that commercial IRBs can be costly and may not have community engagement or members who understand the health center population or needs. Even if health centers do have an IRB, several interviewees mentioned that they may have to “give up” their IRB and use the IRB established by the study sponsor.
Surveyed health centers that engaged in research and that serve a majority of patients living on the lower end of the federal poverty level (FPL) are nearly three times as likely to cite a lack of regulatory, legal, and ethical guidance for patient consent and access to an IRB (27%) as top challenges compared to health centers with patients living on the higher end of the FPL (8% respectively). Health centers that predominately serve Black (5%) and Hispanic (10%) patients are more likely to cite challenges related to access to an IRB compared to health centers that predominately serve white patients (21%).
Erie Family Health Centers created a research governance process
Erie Family Health Centers believes that engagement in well-aligned research is one important way the organization supports progress towards health equity, by ensuring that medical and public health advancements are inclusive of and relevant to the populations they serve. Because of this belief, Erie has participated in research activities and has had a formalized process to review requests to participate in research for over a decade. To ensure meaningful participation, sustainable implementation, and successful partnerships, Erie established a centralized research team five years ago to support the full life cycle of research engagement at Erie. As research is considered a health equity activity at Erie, the research team reports to the senior director of patient programs and health equity. Erie collaborates with local and national research partners including AllianceChicago, academic medical centers, and universities.
Erie has created a process in which potential research partners submit an application to be reviewed by the health center’s Research and Evaluation Committee. For research to be approved, it must be aligned to Erie’s priorities, including the health center’s focus on translational/quality improvement initiatives; evidence-based practices; community-focused, patient-centered research; and enhancement of Erie’s services.14 Another criteria that Erie works with partners to uphold is ensuring that research is resource neutral and does not impede or divert resource from the agency’s primary mission of providing the highest quality primary, behavioral health and dental care to any patient regardless of their ability to pay. If the committee approves an application, the centralized research team assists with project implementation including contracting, orientation of new research partners, workflow development, implementation, and dissemination of results. The review process and centralized team have been critical frameworks for maintaining long standing research partnerships and ensuring research can be sustainability integrated into health center operations.
Technologies used when conducting research
Among the surveyed health centers that are conducting research today, 70% are using electronic health records (EHRs) to collect real-world data. Other top-used technologies include electronic surveys (56%) and computers or tablets that help research participants enter information (52%).
Half of the surveyed health centers use EHRs to recruit patients. However, interviewees noted that EHRs lack data on the drivers of health (also known as social determinants of health), which could be used to help mitigate potential challenges in clinical trial retention. Interviewees also generally noted that interoperability continues to be a challenge, particularly when sharing data across organizations. Making changes to EHRs for research purposes can be financially burdensome and time-consuming. Some interviewees commented that while many health centers in the same geographic region share the same EHR platform, not everyone may be conducting the same research and may not agree to make changes. Clinical trial specific technologies can help mitigate some of these issues.
Interviewed health centers that have been conducting research for a long time have found that a clinical trials management system can make research processes smoother, and a robust data infrastructure and team allows for more targeted recruitment of participants.
Collaborating with health centers on research requires shared decision-making
Health centers that are conducting research sometimes do so on their own, but many partner with other organizations in the research ecosystem (figure 4). Collaborating with others on research allows a variety of stakeholders to bring different skills and perspectives to the project. For example, partners can provide research expertise, infrastructure, technology, and funding to enable health centers to conduct research. Health centers can support knowledge sharing (for example, understanding community needs), patient recruitment and engagement, and study design. Stakeholders approaching health centers as partners should express the shared benefit and value that the research provides by ensuring alignment with health center priorities and patient needs.
In addition to the more traditional partners identified in the survey (figure 4), during interviews we learned about other potential partners including clinical and translational science institutes that provide resources,15 an osteopathic medicine school that incorporates research projects at health centers into their training program, federally funded research and development centers (for example, MITRE which helped pilot and support health centers participating in the All of Us Research Program16), and private funders that contribute to research in innovative and impactful ways.
Collaborating with others on research allows a variety of stakeholders to bring different skills and perspectives to the project.

Academic institutions
Health center leaders who participated in the survey indicated that they are most likely to partner with academic institutions (figure 3). Because some clinicians are both on staff at a health center and affiliated with a university, it can be a natural bridge for collaboration. Universities that already work on research may be able to share the expertise (for example, statistical skills) and infrastructure (for example, physical space and analytics) that health centers lack.
Interviewees noted that despite these sometimes long-standing and amicable relationships, their priorities are often different. For health centers, the focus is on their patients and academics are working to improve patient care but must also publish papers. When staff is not shared across the universities and health centers, academic researchers don’t always fully understand how health centers operate differently from universities. Some interviewees suggested that university staff would benefit from visiting health centers and forming closer relationships with health center staff. In many cases, universities serve as principal investigators in the studies, and health centers serve as sites, but many interviewees expressed interest in being co-principal investigators.
Learning between health centers and universities should be bi-directional. Health centers could educate academic researchers on patient subpopulations, including providing information on patients’ social and economic needs that may impact participant retention in research. Additionally, health center staff members can explain how to gather informed consent from patients, while academic researchers could provide education on navigating grant proposal applications and reporting requirements.
Government entities
After academic institutions, surveyed health centers are most likely to partner with the federal government. Many government entities play a role in the research activities that health centers participate in, particularly in regard to providing funding, infrastructure support, and regulatory guidance.
Health center interviewees involved in government-funded research were grateful for the funding, particularly infrastructure funding (see sidebar, “The Whitman-Walker Institute focuses on building its research infrastructure,” for more information). However, they noted that government grant applications can be difficult for health centers to respond to, and often have exclusion criteria that do not allow health centers to apply as principal investigators. Some of the leaders we spoke with hope that new health center investigators would be able to receive training and early-stage investigator status, or something similar, to help increase health center participation in government-funded research. As one survey participant shared, clearer guidance to “ensure research is conducted in compliance with health center requirements and can be conducted without conflict with billing and cost-reporting" would also be helpful to allow health centers to fulfill their reporting requirements more efficiently.
With the FDA continuing to focus on enhancing the diversity of clinical trial populations17 and the National Institute of Health's (NIH) commitment “to inclusivity in clinical trial research,”18 bringing in health centers seems like a natural fit. As one senior research director commented, “we are currently spending money trying to diversify institutions, rather than investing in places that already have diversity.”
The Whitman-Walker Institute focuses on building its research infrastructure
The Whitman-Walker Institute for research, policy, and education was established in 2018, but the health center has been involved in research since the beginning of the HIV/AIDS epidemic, participating in the original AZT (zidovudine antiretroviral) trials. Since then, clinical trials have been an important part of the organization’s mission to ensure that patients have access to potentially lifesaving medications; Whitman-Walker have studied almost all of the HIV and Hepatitis C medications that are commercially available. Today, the Institute continues to work with pharmaceutical companies, but is also engaged as principal investigators in large federally funded research, with a goal of leading more research in the future.
One such research grant was awarded in October 2022: Whitman-Walker received a $2 million construction award from the NIH to build an HIV biomedical research space.19 The space will be jointly used by Whitman-Walker and George Washington University, with plans to include other research partners in the future. A confluence of factors enabled this opportunity: Whitman-Walker decided to expand its research capabilities and brought in a senior director of research who is affiliated with George Washington University at the same time the NIH released the construction funding opportunity. According to the announcement, this is “a historic investment by NIH to strengthen infrastructure among institutions with a demonstrated mission to serve communities underrepresented in research.”
Pharmaceutical companies
When asked about conducting clinical trials with pharmaceutical companies, most interviewed health centers expressed reluctance. However, when asked about the lack of diversity in clinical trials, interviewees were quick to note the importance and value of ensuring diverse populations are included. We explored this seeming disconnect of partnering with pharmaceutical companies to improve clinical trial diversity.
According to our survey, health centers typically don’t partner with pharmaceutical companies on research. The health center leaders we interviewed shared several reasons for this, including:
- Business structure: Life sciences companies are for-profit organizations, whereas health centers are nonprofit organizations.
- Trust: There’s a legacy of mistrust in clinical research among medically underserved populations (government and academic entities are also impacted by this).
- Work culture: Health centers’ priority is to provide care to their patients and research must fit around that (talking to patients before/after their appointment).
- Ethical concerns:
- Not having access to drugs after a trial has concluded,
- Lack of recourse for research participants if there are negative outcomes, and
- Sensitivity to the perception of coercing patients, particularly when patients only have access to a single health center that is asking them to participate in research.
Despite these obstacles, some interviewees have collaborated with pharmaceutical companies (see sidebar, “Neighborhood Healthcare partners with pharma on clinical research,” for more information), and other interviewees believe more research partnerships between the two are possible. They noted that while health centers are nonprofit entities, they prescribe medications produced by pharmaceutical companies. By participating in clinical trials, health centers could enhance access to new treatments for their patients and generate evidence that proves the safety and efficacy of these treatments for underserved populations.20
Another interviewee noted that while their health center applies for funding from pharmaceutical companies, they make sure that there is a direct benefit to their patients, the funding source does not impact the research, and appropriate disclosures are included when presenting research. Of the interviewees who were open to working with pharmaceutical companies, most agreed that phase 1 and phase 2 clinical trials would be difficult to do, but phase 3 and phase 4 trials were more likely and would make sense to participate in.
To make the partnerships successful, the interviewees noted that sponsors must consider the shared benefits of conducting research with health centers and how partnering helps improve outcomes for their patients. As one research director we interviewed said, “pharmaceutical companies must demonstrate a shared need and what value they add. Their typical approach is not going to do it, but there are win-win opportunities.”
A long-term commitment is necessary, for example, to ensure that patients have access to the drug or intervention after the study ends, health center staff receive ongoing training, and investments in the research infrastructure are made (for example, providing cold storage to health centers). Other interviewees noted that pharmaceutical companies need to be comfortable working with health centers that may have different processes than they are accustomed to. For example, health centers might have a differed process for how they obtain informed consent, design a clinical research protocol, and may be new principal investigators.
Some interviewees were optimistic that by working with pharmaceutical companies, health centers could potentially diversify funding streams, although it would require a few years of investment before showing returns. But not all interviewees agreed with the viability of this approach: Given the amount of work required to set up a study, the fee for service model, and trials that close early, health centers could potentially lose money, they said.
Neighborhood Healthcare partners with pharma on clinical research
Neighborhood Healthcare, a health center located in San Diego and Riverside counties, Calif., has been conducting clinical research for 20 years. One of its first forays into research was as a satellite site for Scripps Research Translational Institute, which they continue to work with. Over time, they have partnered with many others including government entities, universities, and pharmaceutical companies.
One of the health center’s physicians first became interested in participating in pharmaceutical clinical trials and started exploring opportunities. Over time, Neighborhood Healthcare invested in training three of its patient facing employees in research, all of whom are now bilingual study coordinators that report to the chief medical officer. They currently conduct a multitude of phase 3 and 4 studies in areas including diabetes, obesity, COPD, colorectal cancer screenings, and COVID-19 treatment and preventions trials.21
The health center selects which trials to participate in based in part on whether the trials show a clear benefit to their patients, ensure participants are reimbursed appropriately, and/or give access to treatments they wouldn’t otherwise have access to. Neighborhood Healthcare’s data team has been instrumental in helping the research team identify which patients qualify for trials. The health center works with a third party to help administer the trials (for example, contract and regulatory requirements). Neighborhood Healthcare also sees clinical research as a potential way to diversify the health center’s funding streams, however, the revenue is not generated immediately given the time it takes to build the necessary infrastructure.
Neighborhood Healthcare’s C-suite and Board of Directors are fully supportive of taking part in clinical trials because they want to ensure that health center patients are represented, and the medications being studied work for underserved populations. As one of the health center’s leaders told us, “Pharma companies need to give some of these clinics that are interested a chance, even if they don't have extensive clinical trials experience because they are never going to get it unless they are given a chance.’”
How organizations can be better research partners for health centers
Even though each health center is unique, the leaders we interviewed provided several leading practices for potential partners to consider when partnering with health centers:
- Ensure community input: In conjunction with health centers, research partners should include community perspectives throughout the research process, from the determination of research questions to the research protocol, participant-facing materials, and dissemination of research. Partners that attend community meetings and spend time meeting staff and patients at the health center will gain a valuable understanding of community needs.
- Lead with the health center: Health centers should be viewed and treated as equal partners in the research, not simply as recruitment or data sites. Most health centers prefer a collaborative process in which the staff are involved and can learn and provide input rather than feeling as if they are part of an extractive, impersonal relationship.
- Establish realistic timeframes: Working with a new partner takes time, but if the time is spent building trust, future collaborations will likely be easier. Even when health centers have staff focused on research, the on-the-ground work will likely take longer than most research stakeholders are accustomed to.
- Improve the informed consent process: The informed consent process will need to be edited to help ensure that health center participants fully understand what they are signing up for. This will potentially require more time and resources (for example, making forms available in multiple languages).
- Disseminate research to communities: While health centers are sometimes interested in traditional dissemination routes, the process of applying to traditional journals can be cost-prohibitive. Dissemination should also reach back to the community in the ways the community prefers (for example, ask them how they would want to hear about the research findings). Research can be disseminated to the community through reports at regularly scheduled meetings, via newsletters and the local media, social and non-traditional media outlets, and by sharing materials in a public space where community members can walk in and read about the research.
- Give proper credit: Researcher partners using data collected by health centers should acknowledge the source of the data they are using. Too often, researchers publish findings from data collected and entered by health center staff members, but do not share credit with health centers. If health centers are clinical trial sites or serve as principal investigators, they should also be acknowledged in published papers.
- Provide participants with long-term benefits: Once a study is complete, and a medication or intervention works for a patient, how can patients continue to have access to the therapy? Particularly when a drug is not covered under insurance (or the patient doesn’t have insurance) after the drug goes to market, how can research entities ensure patient access to medications long term? These are questions that the research ecosystem should address for underserved research participants.
Additional avenues to conduct research in communities
Retail pharmacies and clinics including Walgreens, Kroger, and Walmart, are also looking to bring clinical trials closer to where patients live and receive care. These companies have major footprints around the country, including in underserved areas, and most Americans live near one of their locations.22
To demonstrate the community-level possibilities, Kroger is recruiting participants for an observational trial on colorectal cancer gut and immune health.23 And Walmart is planning to conduct clinical trials on chronic conditions.24 In June 2023, Walgreens announced its sixth clinical trial partnership which focuses on early detection of cancer.
Elevating communities and health centers within the research ecosystem
The research conducted at health centers tends to be serendipitous, whether it’s a provider’s personal interest driving the investigation or a potential research partner proposing clinical trial participation. Can there be a transition to a more systematic and purpose-driven approach within health center research? And if so, where can it begin?
The path toward enabling health centers to engage effectively in research, especially clinical trials, will likely require a multifaceted approach. It hinges on three pillars: policy transformation, investment in infrastructure, and fostering trusted collaborations with a shared mission.
Policy transformation that supports health center research participation:
- New research funding programs: Establish specialized research funding programs targeting health centers and their unique patient populations.
- Diverse participation requirements: Enforce requirements to ensure diversity in large-scale trials and the valuation of new therapies, considering factors such as, but not limited to, race and ethnicity, sex and gender identity, sexual orientation, disability, income, and community type (rural, urban, etc.).
- Training and loan repayment: Offer training programs and loan repayment options for community health research leaders and staff, encouraging research expertise development.
- Infrastructure and incentive grants: Provide incentive grants to facilitate the setup of research infrastructure in health centers.
- Government task force: Create a task force or advisory board with a dedicated focus on increasing health center and patient participation in research.
- HRSA awards: Recognize and reward research participation by health centers through Health Resources and Services Administration (HRSA) awards.
Infrastructure investment that ensures resources and technology are readily available:
- Improved accessibility: Enhance accessibility of portals to make it easier for health centers and their patients to find research opportunities.
- IRB training and review support: Offer low-cost or no-cost IRB training and review services.
- Technical assistance: Provide technical assistance for data and technology management and integration.
- Research opportunity hub: Create a centralized hub for health centers with vetted research opportunities.
- Research collaboration community: Establish a community platform for interested principal investigators, companies, and research agencies to engage with health centers.
- Research curriculum: Develop a research-focused curriculum, bootcamps, and certificates in collaboration with the National Association for Community Health Centers.
Building relationships and trust for effective partnerships:
- Outreach and education: Conduct outreach and provide educational resources for potential partners to facilitate effective collaboration with health centers.
- Research journal: Establish a journal for disseminating research in community health, showcasing health center contributions.
- Funding guidance: Offer assistance for health centers in assessing and pursuing relevant funding opportunities.
- Awareness promotion: Increase awareness of research participation and opportunities through conference presentations, marketing, communications, and other outreach efforts.
- Diverse partnerships: Foster partnerships with a wide array of research entities to expand collaboration opportunities.
- Research learning collaborative: Create a collaborative platform for health centers to share best practices, experiences, and insights in research.
Engaging directly with communities is essential to improving clinical trial diversity. It is important that research partners involve health centers in all stages of research design and execution to help ensure that research benefits all stakeholders, especially populations that have been historically exploited or excluded from clinical research. Health centers have a unique opportunity to forge new research partnerships that both advance biomedical knowledge and achieve equitable health outcomes for all patients.
Appendix
Survey respondent characteristics:
Region | |
Midwest | 25% |
Northeast | 21% |
South | 28% |
West | 24% |
Other | 1% |
Urban/Rural | |
Urban | 59% |
Rural | 41% |
Insurance Status | |
Medicaid | 47% |
Uninsured | 8% |
FPL Status | |
% FPL | 45% |
Gender distribution | |
Male | 33% |
Female | 46% |
Race/ethnicity | |
White | 38% |
Black | 19% |
Hispanic | 29% |
Others* | 6% |
Health center (average) |
|
Total full-time employees (FTE) | 228 |
Medical care staff | 77 |
Total patient visits | 87,092 |
Virtual visits | 17,710 |
Medicare care visits per total FTE | 250 |
Virtual visits per medical care staff | 208 |
* Others include Asian, Pacific Islander, and Native American
Definition of research used in the survey:25
- Basic or Laboratory Research focuses on understanding the fundamental mechanisms of biology and disease, often using laboratory-based experiments. For example, investigating the underlying biological mechanisms of Alzheimer’s disease in mice.
- Clinical Research: Clinical Trials test interventions such as medications, devices, or procedures by assigning human subjects to different treatment groups. For example, a randomized controlled trial that examines the safety and efficacy of the new drug in patients with Alzheimer's disease.26
- Clinical Research: Observational Studies involve observing groups of human subjects who are already receiving interventions, such as medications or procedures, as part of their usual medical care, to assess their impact. For example, a case-controlled study that observes patients with Alzheimer’s disease who are already taking medication as part of their usual medical care
- Epidemiological Research focuses on the distribution and drivers of health (also known as social determinants of health) across subpopulations and uses observational or analytical methods to identify risk factors or examine patterns of disease. For example, a population-based study that examines the prevalence and incidence of Alzheimer's disease in a specific population, such as older adults in a certain geographic area or demographic group.
- Health Services Research seeks to understand how health care services are delivered, how they are accessed and utilized by patients, and how they can be improved to better meet the needs of individuals and communities. Some examples include annual patient surveys or patient focus groups.
- Participatory Action Research emphasizes the involvement of community members in the research process.
- Research tool design develops and tests tools. For example, the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences.











{kind=link}
{kind=link}
{kind=link}
{kind=link}