The US$2.8 trillion opportunity: How better health for all can drive US economic growth
The Deloitte Center for Health Solutions’ latest analysis reveals how businesses can benefit from a healthier, more productive workforce and contribute to a more equitable society


Kulleni Gebreyes

Jay Bhatt

David Rabinowitz

Michelle A. Williams

Mani Keita

Wendy Gerhardt
Foreword
Businesses can be powerful agents of positive change, and we’ve witnessed firsthand the profound impact that innovation and collaboration can have on our communities. At Deloitte, we lead with purpose to help create a more prosperous and equitable society through our commitments to social impact, sustainability, equity, and trust. We’re not alone in striving to make that aspiration a reality—businesses have long played a significant role in shaping economic, environmental, social, and health landscapes. This broad role of business presents both an opportunity and a responsibility to contribute to a better future.
Health equity discussions typically focus on costs—to individuals, businesses, and the health care system. The economic analysis presented in this Deloitte Center for Health Solutions report suggests that prioritizing health equity could create value and have a positive impact on both our communities and the economy. The modeling highlights how addressing health equity gaps across the United States could add US$2.8 trillion to the US gross domestic product by 2040, representing a 9.5% increase over current economic projections. The benefits for businesses are also substantial, with corporate profits potentially increasing by US$763 billion through the improvement of health equity. Good business and good health for everyone can go hand in hand.
This stakeholder capitalism approach to health equity considers how businesses can create long-term value by addressing not just financial performance, but also environmental, social, and governance (ESG) issues. Deloitte analysis shows that focusing solely on shareholder value has driven significant economic growth and prosperity, but often overlooked the effects on other stakeholders. By considering all stakeholders, businesses can better understand their overall impact and act on opportunities to positively influence the nation’s economy, environment, social factors, and health. Addressing health equity is an opportunity for businesses to make a meaningful impact within this framework.
As leaders, it’s important to commit to bettering the societies and communities where we live and work. We all have a role to play—and an economic opportunity—in driving positive change.
Lara Abrash, chair, Deloitte US
Jason Girzadas, chief executive officer, Deloitte US
Introduction
Health status in the United States varies widely across gender, geography, race, ethnicity, and socioeconomic circumstances, and is impacted by other life experiences and systemic biases.1 The cost of health inequities is substantial, impacting both business performance and the nation’s economic prosperity. According to the Deloitte Center for Health Solutions’ economic analysis, improving health equity across the United States could add US$2.8 trillion to the US gross domestic product by 2040. For US-based businesses, we estimate that corporate profits could increase by U$763 billion in the same time period through more equitable health outcomes (see “Methodology”).
TABLE OF CONTENTS
And according to our research, improving health equity isn’t just a job for the US health care system alone. Public and private organizations could gain from the economic growth and have a direct role to play by making health equity a strategic priority in their workforce resources and operations, products and services, community engagement, and cross-sector collaborations. Sectors such as agriculture, manufacturing, retail, technology, transportation, and many more could reap the commensurate economic benefits that come from a healthier population and workforce. By working to address health gaps, businesses could see improved workforce participation and productivity, significant financial gains, and a more equitable society.
Health inequities are costly
- Systemic costs are increasing. Resources spent on poor outcomes, reduced work productivity, and the financial burdens on individuals due to health disparities appear to be hindering US economic growth. In previous research conducted by the Deloitte Center for Health Solutions and US actuaries, we estimated that direct medical costs associated with health inequities amount to US$320 billion for the health care system and could exceed US$1 trillion by 2040 if the issue is unaddressed.
- Inequities reduce productivity for businesses and the workforce. In prior research by the Meharry Medical College School of Global Health in collaboration with the Deloitte Health Equity Institute, we estimated that mental health and co-occurring physical health inequities cost businesses US$7 billion due to missed work, US$45 billion due to reduced productivity while at work, and US$63 billion due to unemployment.2 Additional research shows that the workforce impacts of various chronic conditions and cancer, which have disproportionate burdens on people from marginalized backgrounds,3 can range from 10% to 70% in productivity loss.4
- Health inequities impact individuals financially. Prior analysis by the Deloitte US actuarial team shows that employed women, on average, pay US$266 more in out-of-pocket spending per year than employed men, which is just over 18% more than men’s out-of-pocket costs, excluding pregnancy-related services. A survey of more than 2,000 US adults conducted by the Deloitte Center for Health Solutions in 2024 shows that women are 30% more likely than men to skip care due to costs and are also more likely (44% vs. 25%) to be financially unprepared for an unexpected US$500 medical emergency.
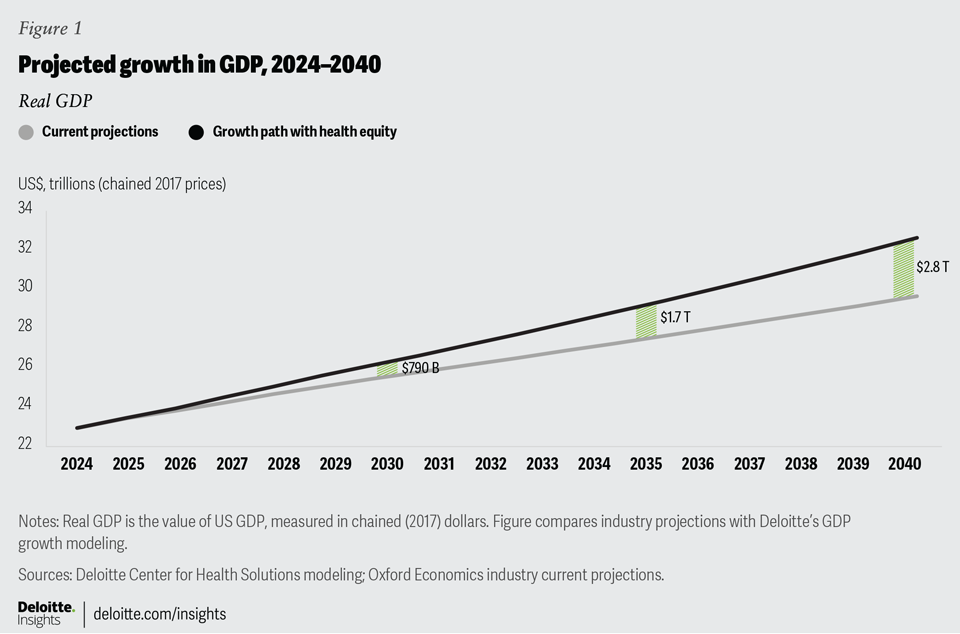
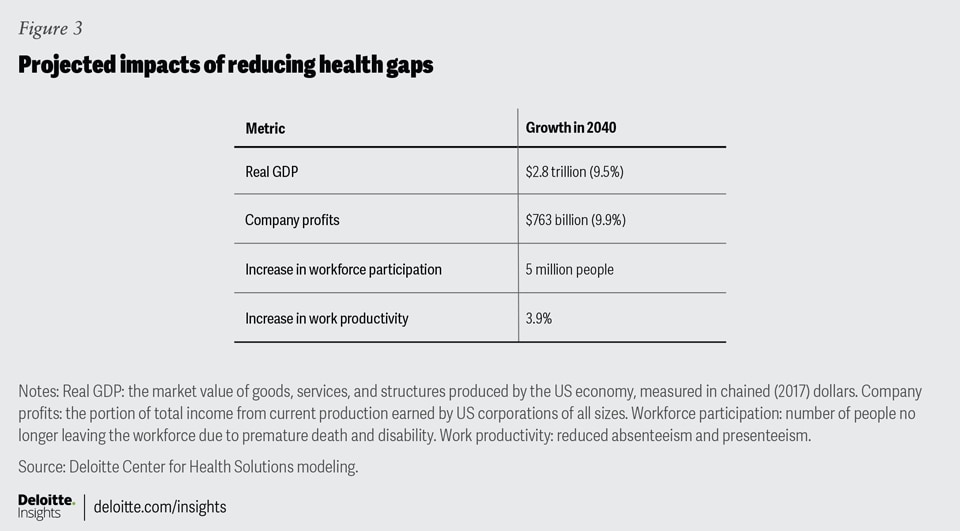
Businesses can achieve growth and value by investing in more affordable, equitable, and effective health solutions. Although these investments require upfront costs, they can ultimately offset the rising expenses that are currently being incurred and are expected to increase over time. Our estimates show that reducing health inequities can create significant economic value, including a gain in GDP and benefits for businesses. By 2040, the potential gains in GDP could reach US$2.8 trillion, including US$763 billion for corporate profits. These figures represent increases of 9.5% and 9.9%, respectively, over current projections (figures 1 and 2).


Additionally, reducing health gaps could prevent five million people from leaving the workforce due to premature death and severe disability (figure 3). Addressing health equity not only can enhance individual well-being, but also can offer substantial economic and business benefits, making it a strategic focus for future growth and success.

The pivotal role of businesses in driving change and reducing costs
Today’s US businesses continue to be impacted by high medical costs, with workforce retention, productivity, and market impact being important for organizational growth and value.5 Healthy employees are more likely to show up for work consistently and perform better.6 For businesses, that tends to mean increased productivity and reduced costs associated with absenteeism and health care needs.
Shifting from treatment to prevention could yield more healthy and productive years
In the Deloitte US vision for the Future of Health, we discuss a change from disease-centered care to well-being-focused care, leveraging innovation and prevention to promote health across people’s life spans. Prior Deloitte Center for Health Solutions research modeled this transition, showing that it could result in each individual adding an average of 12 years to their life span and nearly 20 more years in better health, particularly for those with significant health gaps.
Given the impact of work and employment on health, employers can play an important role in advancing these increases in health and life span. These improvements in healthy years can drive demand for innovative, equitable goods and services aimed at consumer well-being, enabling communities to enhance their lives and contribute productively to society. This shift tends to present businesses with an opportunity to expand their role, scope, and engagement with communities, consumers, and their workforces.
How to generate financial value through health equity
In today’s business landscape, efforts that integrate health equity across organizational activities are not just ethically sound but also tend to be financially beneficial. All US sectors from consumer, technology, energy, health care, government, and more could play a role in helping to improve health equity through their business operations, products and services, community engagement, and ecosystems collaborations.7 Businesses can amplify the momentum of ongoing health equity to think about how to address the inequities in their workforce and communication. Here are a few considerations.
1. Integrate health equity across your workforce, benefits, and programs
It’s important to examine the health gaps and economic costs that may be present within your own workforce to improve your understanding of your own workforce’s needs and inform your approach to more equitable organizational operations—ultimately helping to improve talent retention and productivity.8 By examining your benefits program, it’s possible to mitigate potential organizational inequities. For example, our prior research on the disparities in women’s out-of-pocket health care costs finds potential gender-based inequities in organizations’ average benefit design. This could exacerbate already inequitable income for women in the workforce9 and impact their ability to maintain their health and, subsequently, work productivity.
Understanding the health of your workforce and populations with disproportionate health gaps can support more equitable workplace programs. Over half of US adults have one chronic condition,10 with disproportionate outcomes among marginalized groups.11 Workplace health interventions of various designs focusing on chronic disease risk factors such as stress, diet, and physical activity have been shown to improve behavioral health outcomes.12 In some settings, workplace interventions addressing employees’ health and well-being have decreased organizations’ health care costs by up to 26%.13 However, the design and implementation of these programs is not “one size fits all” and should center on equity to help ensure that they don’t exacerbate poor outcomes.
The complex and varied factors influencing inequities and gaps in health outcomes
Health equity is the fair and just opportunity for all to maximize well-being.14 Inequities and health gaps among populations happen through structural biases and differences in people’s access to and quality of care, as well as social, economic, and environmental factors known as the drivers of health. For example, access to healthy food, digital resources, and transportation, alongside disability status and race are just a few experiences that impact health.15 The range of factors that contribute to health gaps and inequities is extensive, with at least 80% of health being impacted by the drivers of health.16 Regardless of industry, companies have a vested interest in the health of their employees, customers, and communities.
2. Design products and services with equity in mind
Equity-centered design is important for developing products and services that address the needs of diverse populations.17 This involves leveraging a broader range of data sets and includes the experiences of people from different backgrounds so that businesses can better understand and meet the needs of their workforce and community. For example, more inclusive data sources could improve an organization’s understanding of food insecurity or suboptimal nutrition among their target audience,18 thereby enabling them to better tailor their products, pricing, access, and messaging to better meet consumers’ needs and, ultimately, improve health equity via healthy food guidance.
Businesses can also help ensure their products and services are designed with equity in mind by addressing biases in underlying data, such as those found in artificial intelligence systems used for housing and mortgage applications.19 By actively identifying and mitigating these biases, employers can transform these risks into market improvements. For example, there are opportunities to collaborate with community lenders to improve the range of financially inclusive products, promoting equitable access to essential resources and fostering healthier communities.
3. Strengthen your organization’s community engagement
Engaging with local communities and collaborating across sectors can improve health equity and outcomes while also scaling business impact. For example, businesses in rural areas face specific community needs, such as gaps in physical and digital access to health resources, which affect the local population’s health outcomes and life spans.20 Tailoring strategies to local needs can improve community and workforce well-being, and support economic output.
Prior research by Deloitte Center for Health Solutions indicates that successful place-based work relies on forming purposeful and lasting community collaborations, and ensuring community voices are heard and respected. Key elements include promoting community ownership and empowerment, using advanced analytics through technology and key performance indicators to measure progress, and adopting equitable governance models.21
4. Collaborate with sectors across the ecosystem
Beyond making an impact on a local level, sectors can collaborate to leverage each other’s strengths and resources for greater scale. Multisectoral collaborations provide valuable resources to guide organizations in working within and outside of their sector to improve health equity and enhancing economic value.22
Stakeholders can also leverage regulatory initiatives, such as the White House’s focus on women’s health research, to better facilitate and inform their work for specific populations.23 State-level efforts or resources, like information on community engagement in Virginia or place-based activity in Washington, offer additional opportunities to advance multisector relationships and leverage ecosystem resources to drive both health equity and sustainable growth opportunities.24
In an era in which business growth, talent retention, and productivity are top concerns for many C-suite executives,25 health equity has emerged as an influential driver of all of the above, according to our research. Whether focusing internally or externally, within health care or across various sectors, advancing health equity is a business imperative and could help foster a more prosperous society.
Methodology
Step 1: Measure differences in health outcomes
We examined the landscape of inequities among populations and measured differences in health outcomes (disease prevalence and mortality, years of life lost, and years lived with disability) across various population cohorts. We focused on 12 key public health concerns: asthma, breast cancer, colorectal cancer, diabetes, heart disease, homicide, maternal morbidity and mortality, mental illness, musculoskeletal disorders, stroke, substance abuse, and suicide. The selection was guided by literature on disparities, disease prevalence, and mortality, and discussions with external subject matter specialists in economics and health equity. We calculated disease prevalence and mortality from a combination of data sets including those from the World Health Organization’s Global Burden of Disease (2019), Wonder data from the Centers for Disease Control and Prevention (2018-2021), and Komodo Healthcare Map (2018–2021).26
Step 2: Estimate the impact of bridging health gaps on workforce participation and productivity
We identified four ways that improving health equity can lead to better workforce participation and productivity (figure 4). We employed data from the Bureau of Labor Statistics (2022), the US Census (2020-2022), and secondary literature on labor force statistics and work productivity loss (absenteeism and presenteeism).27 We used race agnostic workforce data on participation and unemployment rates, to account for inherent biases that affect certain populations’ ability to work.

We estimated an 80% improvement of the gaps in health outcomes, reflecting the impact of drivers of health, health systems gaps, and systemic bias on disease prevalence, morbidity, and mortality.28 To identify bridgeable gaps among population groups, we explored various scenarios with different benchmarks and measurements for improvement. These scenarios illustrate diverse ways to measure and bridge gaps, recognizing that improvements vary across population groups. Our model focuses on groups with readily available data, though many identities experience differences in health outcomes.
- Intersectionality and drivers of health: Because of varied experiences within populations, we estimated improvements for all populations regardless of race, relative to the racial group with the leading national health outcomes.
- Systemic racial biases: We estimated improvements for racially minoritized populations, comparing them to the racial group with leading national health outcomes.
- Place-based effects: Using the population group with leading health outcomes from the six US states with the highest life expectancy29 (California, Hawaii, Massachusetts, Minnesota, New Hampshire, and Washington), we estimated improvements for all populations below the benchmark.
- All scenarios control for gender and age (10-year age bands, and larger for older adults).
Step 3: Quantify the economic impact
We used the Oxford Economics’ Global Economic Model, structural and international macroeconomic model, to estimate the impacts on the US economy.30 By incorporating our calculated changes in productivity and workforce participation into the model, we were able to estimate the economic impact of reducing health inequities, measured across several key macroeconomic indicators. We projected out our estimates to 2040 to capture the cumulative progress in bridging health outcome gaps and the compounded gains over time (figure 5).

Step 4: Validate the research approach
We asked 19 leaders in health equity, health economics, policymaking, academia, health care, life sciences, and business to review our analysis for a broader perspective. They agreed that a macroscopic view enhances the accuracy and impact of our findings, providing actionable insights across more sectors.
Reviewers noted that while economic methods can quantify certain aspects, many significant intangible benefits, such as the societal impact of improved health, are harder to measure. They also highlighted potential savings from reduced medical debt and health care costs, though initial health care costs may rise as people live healthier and longer lives.
Study considerations
Research scope
- The primary component of inequality analyzed in this analysis is race, while controlling for age and gender. There are a multitude of factors that intersect and have a compounded effect on health: immigration status, income, language literacy, sexual orientation, urban/rural status, veteran status, etc.
- The goal of the various scenarios is to examine different benchmarks for improvements, and how different ways of bridging inequities can yield potential economic growth. The primary scenario featuring aggregate highest state-level life expectancy is not intended to measure the deterministic impact of specific factors leading to life expectancy. It is to estimate improvements using more local benchmarks, as opposed to national benchmarks.
- This study estimates the economic impact of reducing health inequality but does not currently estimate or account for investments required to bring about such an improvement in health outcomes. As such, it is not a cost-benefit analysis, nor does it examine the opportunity costs of such a use of resources to reduce health inequities.
Modeling assumptions and limitations
- The modeling is done at the macroeconomic level to understand societal gains and does not provide results at a more granular level. While the model includes over 1,000 indicators for the US economic, model assumptions do not fully reflect the complexity of societal decisions and real-world economic systems.
- Owing to gaps in available data, not all inequality was captured. At the time of our study, the Global Burden of Disease data available was from 2019, so it does not incorporate any potential effects of the COVID-19 pandemic on overall disease levels. The exacerbation of COVID-19 on health inequities could suggest higher prevalence and mortality and an underestimation of our findings.31
- Furthermore, each data set has limitations in its completion and missingness.
How the model generates conservative estimates
We believe this model generates conservative estimates in a few ways.
- Measuring health gaps: First, we recognize that certain conditions are underdiagnosed, impacting morbidity and mortality rates.32 Second, closing the gap to just 80% still leaves some unaddressed inequities. Given the relationship between stress and health,33 even differences in biology can stem from stressors due to inequities in the medical and nonmedical drivers of health. Additionally, given potential gaps among identities for which data is limited, there are likely more improvements to account for among populations.
- Estimating economic impacts: First, we recognize that there are secondary and indirect economic impacts when people live longer and in better health (for example, they invest in education, which unlocks more career opportunities, more wealth, and so on). Second, with reduced health inequities, the US economy would likely benefit from any related improvements in consumer medical debt. Finally, some caregiving work could be allocated to other activities, thereby potentially boosting productivity in other ways.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}