What’s causing US women to skip or delay medical care?
A new Deloitte survey indicates three issues could impede US health care progress in helping women lead longer, healthier lives


Kulleni Gebreyes

Jennifer Radin

Asif Dhar

Jay Bhatt

Wendy Gerhardt

Leslie Korenda
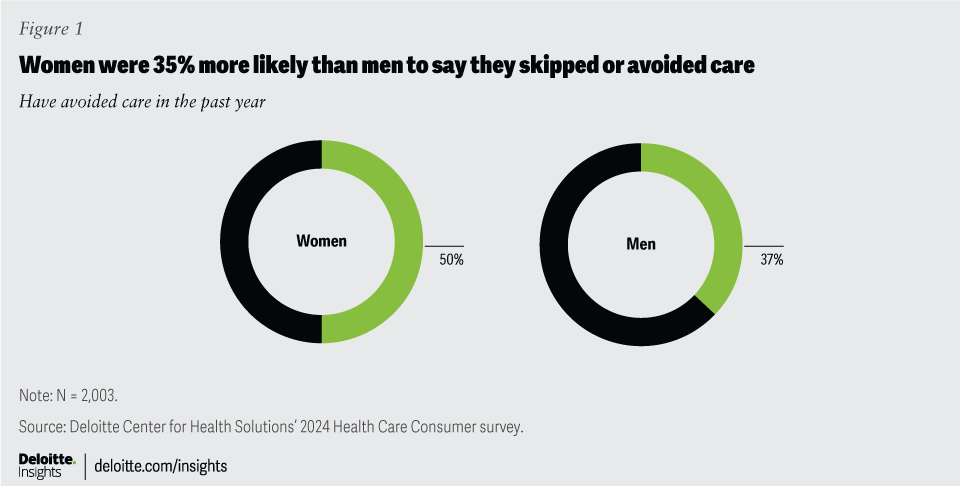
The US health care system may not be fully meeting the needs of women,1 and new Deloitte research reveals what could be limiting women’s use of health care services—and what can be done about it. In a survey of US consumers conducted by the Deloitte Center for Health Solutions, women are 35% more likely than men to say they’ve skipped or delayed medical care over a 12-month period. This potentially leaves their conditions untreated for longer and can compound the costs incurred at the individual, organizational, and societal levels.
In February 2024, the Deloitte Center for Health Solutions asked a nationally representative sample of about 2,000 US consumers how the United States might achieve high-quality health care for everyone, regardless of gender. The 2024 Deloitte Health Care Consumer Survey—the research center’s 12th consumer survey since 2008—found three design flaws in the US health care system that can present formidable barriers to people receiving optimal care, and which disproportionately affect women. These issues offer a possible road map to addressing gender-based inequities in health care—and improving well-being and prosperity more broadly by preventing common ripple effects on women’s families and employers, and on the US health care system itself.2
(The 2024 Deloitte Health Care Consumer survey was inclusive of all gender identities; however, the sample size was not large enough for analysis of individuals who identify as transgender men, transgender women, agender, or nonbinary.)
How women are using—or forgoing—health care services
In addition to our survey of US consumers, we conducted an actuarial analysis of medical claims data to isolate health conditions that are unique to or more predominant in men or women. The analysis concluded that women require an average of 9.9% more health care services than men—even when excluding maternity-related health care expenses,3 This difference could be due to a variety of biological differences or disease prevalence. Women, for example, are more likely than men to be affected by autoimmune disorders4 and Alzheimer’s disease.5 Some health conditions, like heart disease, affect men and women differently.6
The US health care system was originally developed using data and evidence primarily derived from male subjects.7 As such, many medications, treatments, and medical devices have been developed with male biology in mind.8 As a result, women’s health needs have historically been underprioritized and limited in scope.9 But there are signs of progress: Take venture funding, for example, where there’s a growing focus on investment in women’s health initiatives—although challenges persist.10
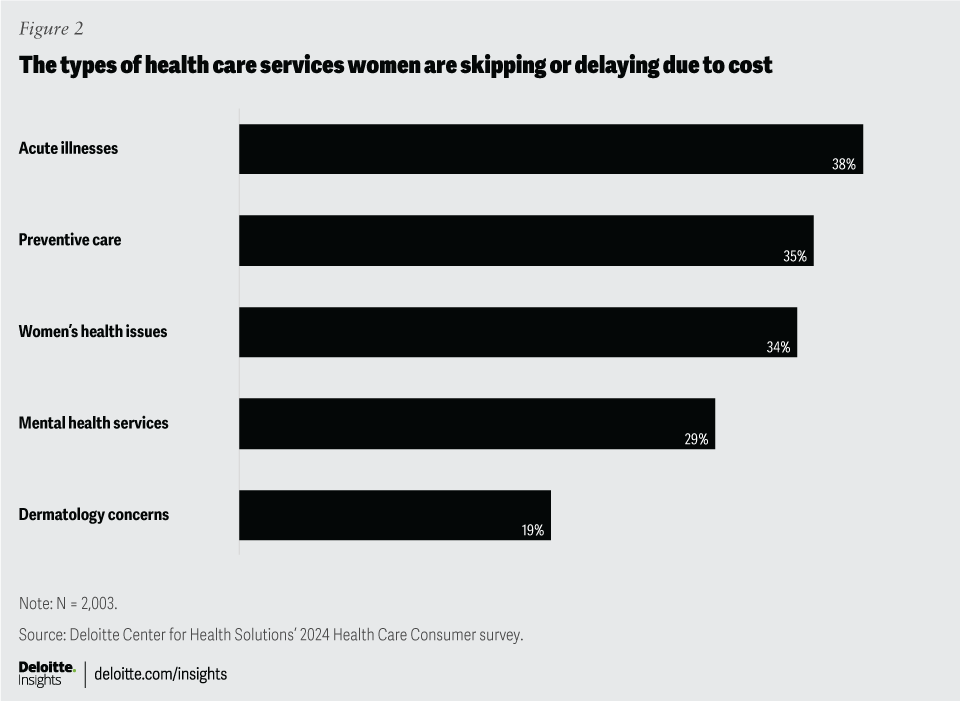
As highlighted in our survey, there is a significant gender disparity in the use of health care services.11 While we shared that 50% of women surveyed (versus 37% of men) have reported delaying or skipping any kind of health care services in a 12-month period (figure 1), we also took an in-depth look into the types of services they’re forgoing. The most frequently missed health care service for both men and women was treatment for acute illnesses such as the flu or a viral infection (38% for women and 37% for men). In addition, 34% of the women we surveyed reported delaying or skipping a women’s health visit (for screenings or maternal health, obstetrics, or gynecology needs) but only 19% reported delaying or skipping a dermatology visit (figure 2). Although not studied by our survey design, women are also more likely than men to forgo prescription medications, according to the Centers for Disease Control and Prevention.12

Avoiding or delaying routine care or not adhering to prescribed medications can result in the deterioration of health conditions, exacerbation of chronic illnesses, and missed opportunities for early diagnosis of treatable and preventable diseases.13 People who miss or delay routine care might require more intensive treatments or emergency interventions in high-cost health care settings. This can lead to an escalation in both the severity of health issues and the associated costs of treatment.14
Preventive services can help people maintain or improve their health by keeping illnesses from developing or progressing into more complicated and costly conditions. And yet, about one-third of survey respondents (both men and women) said they had gone without preventive services, such as vaccinations and cancer screenings, during the past year (figure 2).

Our survey also found that women are more likely than men to avoid or delay mental health services due to cost—29% for women, compared to 22% for men. Some mental health disorders such as anxiety and depression are more common among women than men and others like perinatal depression and premenstrual dysphoric disorders only affect women.15 These conditions could be exacerbated if necessary mental health care is skipped because it is unaffordable or inaccessible.16 This could lead to more care being needed in higher-cost settings.
We also found that younger people, regardless of gender, are more likely to skip mental health care. But choosing to decline care due to cost varied among the generations surveyed. While 47% of Generation Z (born 1997 and later) respondents said they had skipped mental health services due to cost, just 19% of Generation X (born 1965 to 1981) respondents did.
Three structural design flaws may cause women to defer or skip care
It should be noted that women tend to have more health-related appointments than men, according to data from the National Center for Health Statistics, as well as Deloitte’s actuarial analysis. This may be one reason why more women than men in our survey reported they have skipped or delayed care. (In other words, women may have had more appointments to begin with, which presented more instances in which they may have skipped or delayed care in a given year.)
That said, based on our research and analysis, there are three factors about health care that seem to be driving much of the gender inequities and that, if addressed, could yield higher-quality health outcomes, regardless of gender.
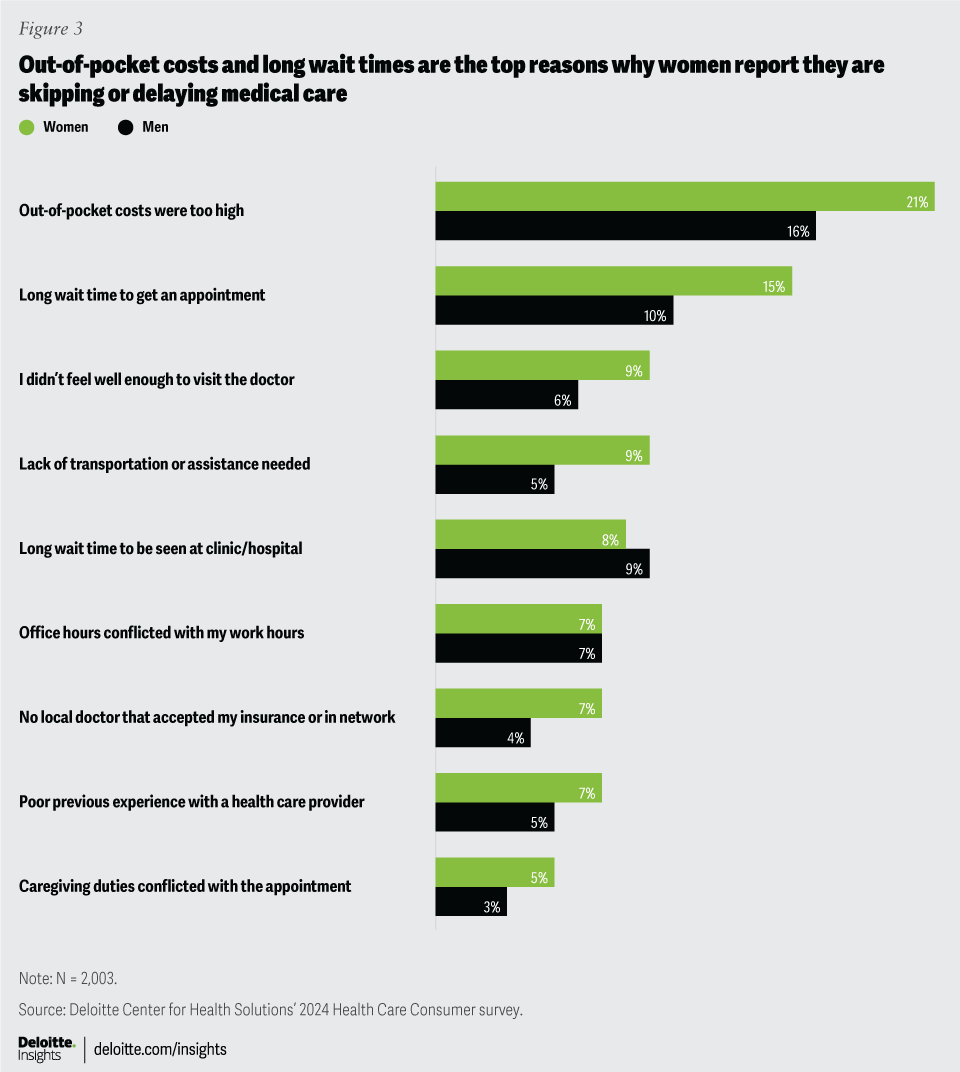
1. Affordability: Women are 31% more likely than men to skip care due to cost, according to our survey results (figure 3). And 21% of women decided not to see a doctor because the cost was too high—up from 15% in 2015.17 Moreover, surveyed women were almost twice as likely as men to say they aren’t financially prepared to pay an unforeseen medical bill. Such expenses could have a more profound impact on women; 44% of surveyed women said they are “not prepared” or “slightly prepared” to pay US$500 for an unexpected medical emergency—up from 37% two years ago. By contrast, 25% of men said they are not prepared to pay for an unexpected medical emergency this year—up from 19% in 2022.18
According to Deloitte’s recent analysis of women’s health inequities, women spend 20% more on out-of-pocket costs—based on their covered benefits—than men. Even after excluding maternity expenses, employed women still spend 18% more than men on health care, which works out to about US$265 a year.19 Women in the United States earn an average of 82 cents for every dollar a man earns and therefore might be less able to cover out-of-pocket expenses.20

2. Access: Women are 50% more likely than men to report skipping care due to a long wait time and are twice as likely to miss a medical appointment because of a transportation issue. Some respondents also said scheduling challenges and long wait times made it difficult to make or keep medical appointments.
However, our survey data also suggests that all consumers may be looking for ways to make care more accessible, particularly women. Among women who have participated in a virtual health visit, 80% said convenience and access were their top reasons for the choice. About 45% of women respondents said the virtual care option offered more convenient appointments; 19% said appointments were less time-consuming; and 17% said it was easier to book an appointment. Unaffordable costs can also make health care less accessible for everyone, particularly for women who earn less on average than men.21
3. Prior experiences: Health care is shaped by data and evidence, but it also relies on assumptions.22 When symptoms for a woman don’t match the established data (which is typically based upon men), patients could be misdiagnosed or ignored. Additionally, taking the time to build trust and listen to community voices is important but frequently overlooked.23 For example, in focus groups conducted in a previous Deloitte US study, more than 40% of female participants said they had skipped or avoided care because they didn’t like the way a provider or a staff member treated them.24 Some of the women participants said clinicians discounted their symptoms, didn’t listen to their concerns, or misdiagnosed a health issue.25 Such interactions with health care providers can create negative experiences that could erode trust and lead women to avoid necessary care.
Women’s distinct health care needs are often unaddressed
Much of women’s health care is confined to what’s known as bikini medicine (for example, breast cancer, reproductive health, and contraception treatments and needs).26 But women’s health extends beyond the parts of the body a bikini would cover. Limited understanding and a narrow view of women’s health care needs can keep some women from receiving the appropriate treatment at the appropriate time, affecting the whole body.
Preventive care for women is predominantly focused on reproductive health and the early detection of breast cancer, cervical cancer, and uterine cancer.27 But cardiovascular disease, not cancer, is the leading cause of death for women.28 Symptoms of heart disease that are specific to women can be more difficult for clinicians, first responders, or patients to recognize due to ingrained misconceptions because the typical heart disease symptoms of men, which are different from the typical symptoms of women, are taught as the standard in medical school and are the basis for interventions and training.29 For example, a man with heart disease might show up at a hospital with chest pain, while a woman with the same condition might have subtler symptoms, such as indigestion or back pain.30
Moreover, women are an average of 4.5 years older than men by the time they are diagnosed with many of the same diseases. And in cases of cancer, men are diagnosed an average of 2.5 years earlier than women, according to a study of nearly 7 million people.31 Another study found that middle-aged women who have symptoms of heart disease are twice as likely as men to be misdiagnosed.32
Can stakeholders help bridge the gender gap?
An equitable US health care system that better supports the needs of women could help universally improve health outcomes. Industry stakeholders can be pivotal in developing strategies that increase the focus on women’s health, remove systemic and structural barriers, and help address unmet health needs with innovative products and services. This could help ensure that everyone has equitable access to health care and the opportunity to achieve similar health outcomes.
By using equitable design and including women and their health needs, stakeholders might be able to make health care more affordable and accessible while improving the patient experience. The concept of equity-centered design seeks to create a more equitable health care system by acknowledging that men and women have different health care needs and varied life experiences.33 It also taps into the voice of the community.34 This approach could help stakeholders address structural design flaws and help bridge the growing gender equity gap in health care.35 It could also help rebuild trust in the health care system. Stakeholders can help address challenges for women by addressing affordability, access, and experience.
What’s the difference between equity, equality, and disparities?
The terms equality and equity are sometimes used interchangeably. However, equality means everyone receives the same resources and opportunities regardless of variations in need or circumstances and despite any inherent differences. In a one-size-fits-all health care model, equality has the potential to create advantages or disadvantages depending on the standard that is used as the default. Equity, by contrast, considers the specific needs or circumstances of a person or group to help ensure they have the necessary resources that take these differences into account. Differences in health outcomes across population groups are referred to as health disparities. Health disparities that are not biologically predetermined and have addressable barriers or root causes—often stemming from structural, social, economic, and environmental drivers—are called health inequities.36
Employers: Employers can play a role in improving workforce health by promoting health literacy, prioritizing well-being, and increasing access to preventive screenings. They can also improve health care affordability and access for women by collaborating with health plans to enhance coverage for health issues beyond fertility and childbirth, such as screenings, rehabilitation therapy, mental health services, and menopause treatments. Additionally, helping to ensure that health benefit options are affordable and meet women’s needs can attract and retain talent while keeping them healthy and productive. Employers could also explore ways to make health care services more accessible through flexible work schedules, onsite health care services, subsidized child care, and paid sick leave.
Health plans: Health plans can play a role in bridging the gender equity gap in health care by addressing affordability, access, and experience disparities. They can start by examining their plan designs for gender biases and introducing new products that equally benefit genders, with a particular focus on women-specific health care needs. Adjusting cost-sharing mechanisms to be more inclusive can also promote equity, with potential changes costing as little as US$1 to US$10 per member per month.37
Additionally, health plans could help employers select plans that align with both their financial goals and equity objectives, while negotiating more affordable rates with network providers for health care services frequently used by women. Increasing gender diversity among decision-makers and incorporating gender-specific cost estimates into cost-transparency tools are further steps that can help develop more equitable health plans.
Hospitals and health systems: Hospitals and health systems could enhance care for women by addressing systemic and structural challenges through several strategic initiatives. Investing in alternative sites of care and other low-cost settings such as virtual visits and retail care locations can help improve accessibility. Customizing care and treatment plans to meet the unique needs of women can personalize and improve care delivery. Improving the patient experience is important; implementing feedback mechanisms can ensure respectful treatment, according to the results of our 2022 US Health Care Consumer Survey.38 Encouraging clinicians to listen actively and educate women about their health can help them make more informed choices about their care.
In addition, addressing unconscious bias through open conversations among staff can lead to more inclusive and equitable care environments. Prioritizing workforce diversity by supporting gender-diverse care teams could enhance understanding and empathy, potentially improving diagnosis and treatment. Additionally, designing digital tools equitably and helping to ensure they address concerns that women have about privacy and trust can increase overall confidence in using technology to manage health needs. Deloitte’s prior research has shown that women tend to be less trusting of technology, less interested in data-sharing, and more concerned about privacy than men.39
Innovators and investors: Despite a 27% decline in overall venture funding from 2022 to 2023, investments in women’s health technologies grew by 5%, marking a difference of 32 percentage points.40 Given the trend, investors should focus on further funding products and services dedicated to women’s health. Adopting a women-centered design approach, especially by involving women directly affected by specific conditions or diseases in the products and services development process, has the potential to lead to further products and services dedicated to women’s health. Additionally, enhancing product design and development through the inclusion of community voices and diverse teams could lead to more innovative and inclusive health solutions.
Other stakeholders, including pharmaceutical manufacturers, medical device companies, and boards of directors can play a role in reducing the gender equity gap in health care. For example, about 4% of all biopharma research and development spending goes toward specific conditions of women.41 Just two out of 37 prescription drugs approved in 2022 were for specific health conditions of women.42 Gender-agnostic drug dosing can further contribute to negative experiences for women. Recommended doses for most medications—including aspirin and other commonly used drugs—are based upon the results of clinical trials that were conducted primarily on men.43
Sponsors of clinical trials could similarly help boost gender diversity in research by including more women. Researchers and institutions should further support diverse teams of investigators and scientists in research leadership roles. Boards of directors could also play an important role in this process by overseeing organizations’ efforts to remain accountable, manage budgets, measure progress, and evaluate initiatives around research and innovations. They could focus on diverse representation within the boardrooms and consider a diverse set of community voices in the efforts.
Addressing the US gender equity gap in health care
While the US health care system hasn’t historically resulted in equitable outcomes for women,44 there are some indicators that might be changing. A few recent federal initiatives could help stimulate interest and investments in women’s health. The White House issued an executive order in March 2024, expanding the federal government’s research on women’s health issues. Complementing this, the National Institutes of Health was directed to spend US$200 million for a new research program that spans the agency’s various institutes. This initiative is focused on understanding the effects of women’s cardiovascular and neurological health.45
Women can be leaders, employees, community members, caregivers, and consumers, among many other roles. They make up nearly 60% of the paid workforce and 65% of the unpaid workforce in the United States, often undertaking the bulk of family health care decisions and serving as caregivers for children and other family members.46 These roles highlight the important need to address gender-based inequities in health care. By focusing on these disparities, the overall well-being and economic prosperity of communities can be enhanced, and the potential for widespread consequences on families, employers, and the broader US health care system itself can be mitigated. This shift toward focusing more on women’s health could not only help bridge the gender gap in health care but also transform the landscape of US health care, leading to a healthier, more equitable future.













{kind=link}
{kind=link}
{kind=link}