Independents who have adopted new models say the workflow should allow for a mix of appointment, walk-in, and virtual customer interactions. One example of a simple workflow modification is medication synchronization: When a patient picks up all their medicines together, it can be an opportunity to discuss how to take them, how they may interact, review their other OTC drugs and supplements, and offer suggestions. Other changes with workflow implications may involve sending a text reminder about medication pickup; alerting patients about a pharmacist counselling opportunity; or even offering the option to schedule the counseling session, receive it on a walk-in basis, or decline.
Developing clinical services and prioritizing them over dispensing could be a big shift for many businesses, both culturally and operationally. They should ensure that pharmacy staff are prepared and supported to make this transformation.
Revenue models that monetize clinical activities and generate value for the system
The Thrifty White example (case study 1) and others like it demonstrate that value-based arrangements between community pharmacies and payers are possible. They may involve per-member per-month payments or direct contracting. Additional revenue opportunities for community pharmacies may be in:
- Long-term care pharmacy consulting
- Relationships with local employers around care management, worksite clinics, or large-scale events, such as health fairs or vaccination clinics
- Opportunities that leverage scope or practice flexibilities at the state level, such as point-of-care testing and prescribing (see Appendix)
Technology supporting workflow and business model transformation
Technology needs to deliver multiple capabilities: Exchange clinical information and connect to EHRs; support decision-making; and automate dispensing, clinical, and administrative activities that are patient-facing, payer-facing, or required for contracting or reporting.
Below are a few examples of technological solutions and concepts we heard about in our research.
- Analytic tools are used across different settings. Risk stratification algorithms identify patients at risk of medication-related events. Other tools estimate drug risks from combining multiple medications as opposed to pair-wise drug-drug interactions.
- At one pharmacy chain, a clinical rules engine pre-identifies most of the medication therapy problems; so when a pharmacist talks to the patient, she can uncover things that are not in the dispensing or drug history data. A team of clinical pharmacists regularly evaluates the clinical rules and identifies new types of signals or events that should be tracked in the data and flagged for frontline pharmacists.
- For pharmacists who have been dispensing for much of their career, clinical decision support can help them transition into clinical services. It can give them the assurance that they are following the latest, most appropriate clinical guidelines. At the same time, it can ensure that across the organization or network, pharmacists deliver consistent services with minimal clinical variation.
- Interoperability solutions bring patient health information within pharmacists’ reach.
- One respondent said that recent e-prescribing standards offer a backdoor channel to digitize communications with prescribing physicians. They have leveraged the connection with the prescribers’ EHR to recommend therapy changes so that the prescriber can act on them sooner. For example, start, stop, or change a therapy or modify the dose.
- Today, pharmacy metrics are not standardized and come with delays, making it hard to enter value-based care arrangements with payers. Some innovators are developing ways to connect pharmacy systems to sources of patient data, leveraging new interoperability standards, and providing monthly performance feedback (see Appendix).
- Smart medication packaging can support medication adherence monitoring in real time. The technology involves blister packaging with embedded electronic chips and a gateway device in the patient’s home that transmits data to the pharmacy. A low energy Bluetooth chip that communicates with the gateway device alerts the pharmacist when the wrong bubble is popped, a package isn’t opened by a certain time, or when medications that should have been discontinued are opened. This triggers a text or phone call to the patient and/or their caregiver.
- We heard that central fill may finally be gaining momentum in community pharmacy. A central fill pharmacy serves multiple retail locations by centralizing drug fulfillment on behalf of the originating pharmacy, mainly for maintenance medications. The medications are then delivered to the originating pharmacy or to patients’ homes. Central fill works best in a hub-and-spoke model and uses automation to process high volumes. The benefits are more time for retail pharmacists to perform other services, reduced inventory costs, lower costs to fill prescriptions, and increased accuracy of dispensing.
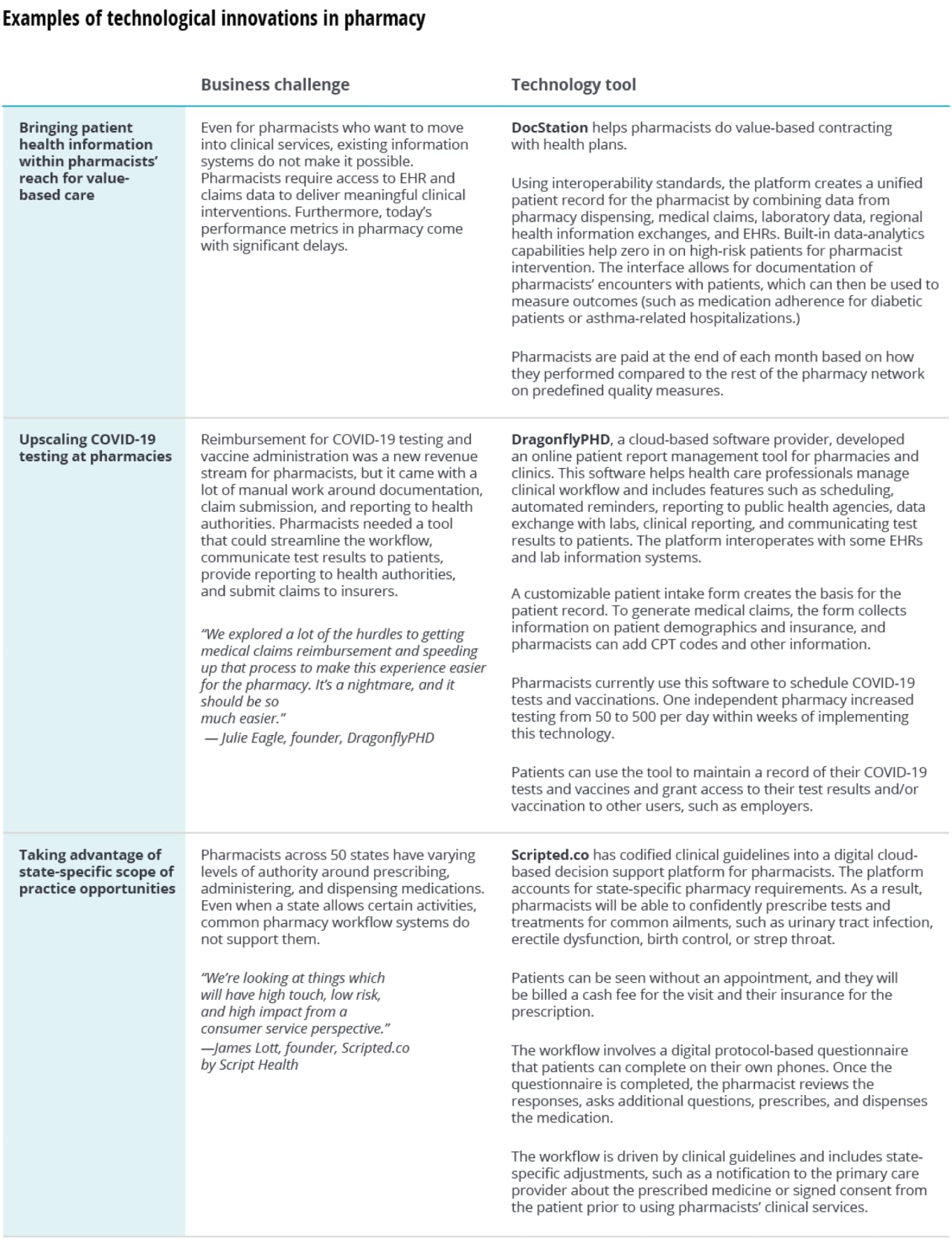
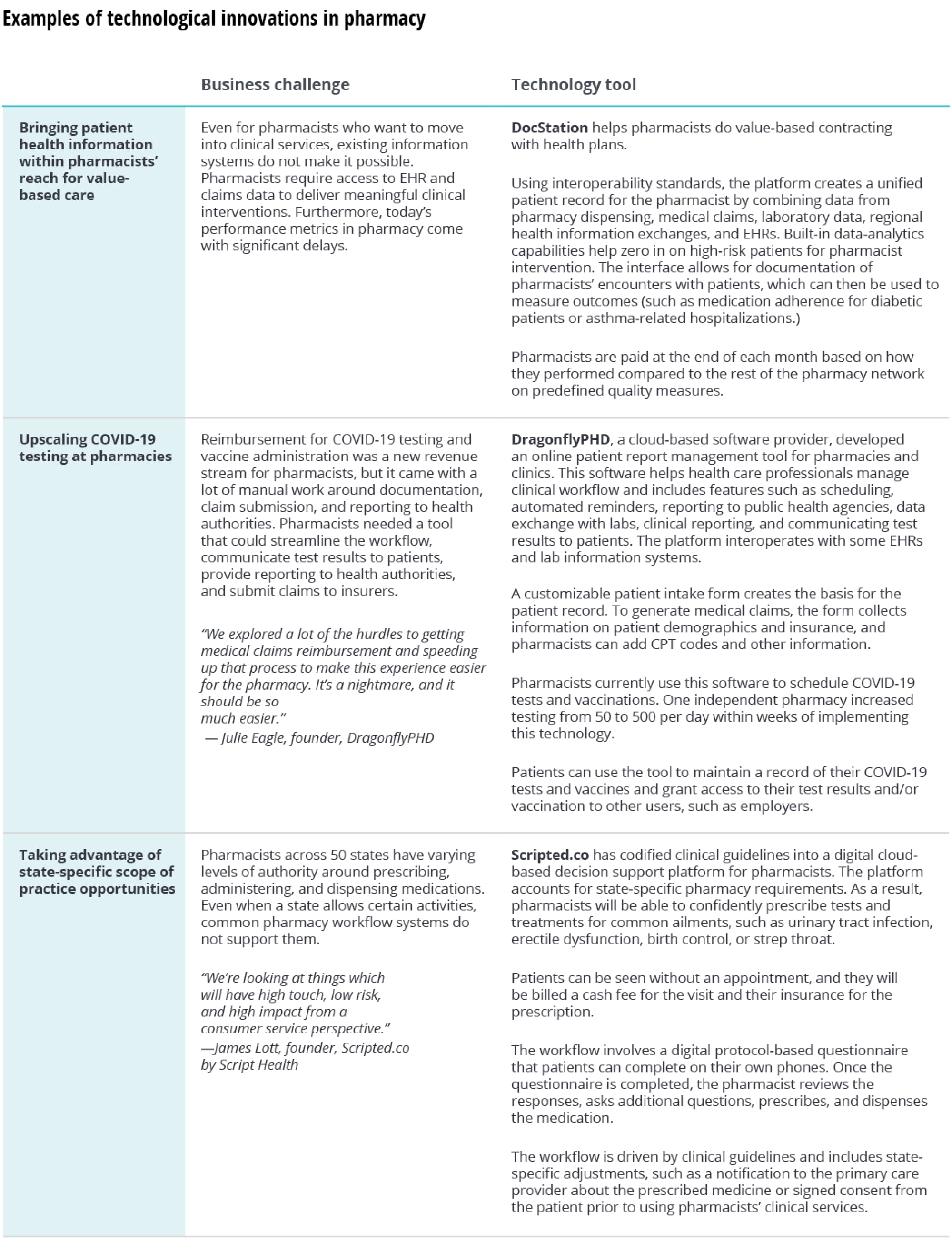
Some technology developers aim to shorten the time to ROI for pharmacies by allowing for new revenue opportunities within months of implementing new technology. In the Appendix, we provide a few examples of technology-based solutions that aim to do just that. These innovators focus on both technology and business side, developing solutions that address pharmacist workflow, decision support, revenue generation, and accounting for state-level disparities in regulatory requirements and scope of practice.
Rethinking the pharmacy model: Provider setting
Experience from Geisinger's (case study 2) and others’ success at incorporating pharmacists into care teams offers lessons.29 We suggest that organizations start with an assessment of their existing service lines, growth plans, and quality performance to identify areas where adding or reallocating pharmacy resources would make the most sense. For instance, in primary care, embedding pharmacists in patient-centered medical homes or collaborating with community pharmacies might be a consideration. For inpatient services, transitions of care and reduction in readmissions may be valuable.
Below we offer a few considerations for provider organizations around workflow and staffing, revenue and cost, and technology that we heard about in our research.
Workflow and staffing
In ambulatory settings, workflow should enable pharmacists to be part of care teams and support care transitions and communications with community pharmacists. At large health systems, pharmacists embedded in ambulatory care teams can be shared by several practices and many pharmacist consultations can be virtual. Our participants also had some advice. In-person pharmacist-patient interactions are valuable at the outset because they help establish trust and rapport. Another good practice is continuity of relationships: In their experience, patients who saw the same pharmacist had significantly better outcomes than those who bounced around between different pharmacists.
Not all physician practices can add pharmacists to their staff, as pharmacists can be at least as expensive as nurse-practitioners or physician assistants. Even health systems with large pharmacy resources may find value in working with local community pharmacies, especially around care transitions from inpatient into community or long-term care settings. Developing robust communication and information exchange processes is critical in such collaborations. One pharmacy owner who has partnered with academic clinics uncovered considerable information gaps on both sides and said, “by communicating and collaborating we could optimize medications better than if we were trying to do this alone.”
Revenue and cost considerations
Some pharmacy investments could support revenue generation, others could lead to cost savings; in many cases, it would probably be a mix. Existing and future arrangements with payers could inform where to invest, and new types of contracts may be needed. Collaborations with community pharmacists, or even in-house pharmacists, may require collaborative practice agreements and three-way arrangements with payers, with shared savings or bonuses tied to outcomes like hospital admissions or ER visits, as well as new patient attribution models. Internally, organizations may choose to measure additional outcomes, such as patient and clinician satisfaction, changes in panel size, wait times for specialist appointments, or resource utilization.













{kind=link}
{kind=link}