






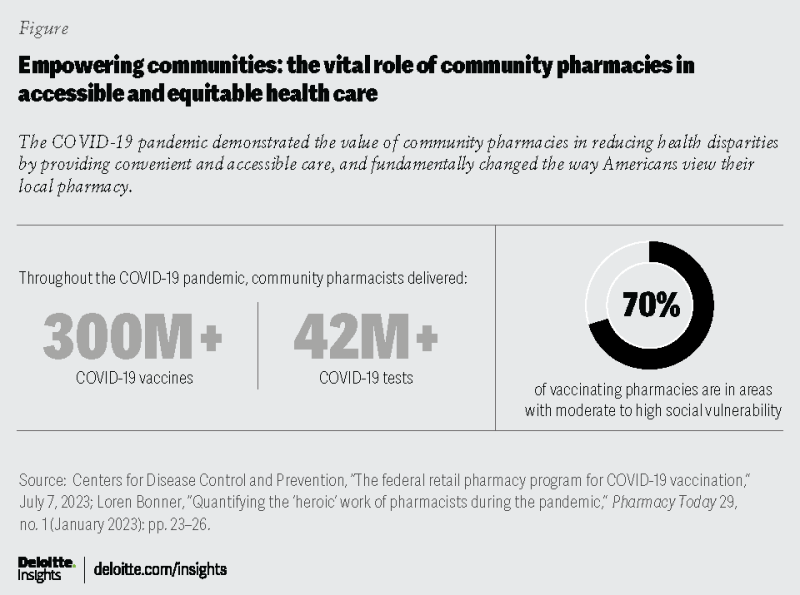








The role community pharmacies can play in reducing health inequities has been saved
Project team: Apoorva Singh and Dimple Jobanputra conducted the case study analysis, secondary research, and project management. Greg Myers provided invaluable guidance on shaping the research.
The authors would like to thank Reena Kersch, Andrea Schiff, Vipul Bhatt, Wendy Gerhardt, Jay Bhatt, Chelsie White, Ryder Riess, and Linda DaSilva for their insights, expertise, and critical feedback on the research. Rebecca Knutsen, Laura DeSimio, Melissa Williams, Julie Landmesser, Zion Bereket, Kim Cordes, and many others contributed to the success of this project.
This study would not have been possible without our research respondents who graciously agreed to participate in the interviews. They were generous with their time and insights.
Alex Jung, managing director, Parthenon EY; and former senior vice president, Corporate Strategy, Walgreens
Alyssa Zarzecki, pharmacy manager, Sam's Club
Andrew Gentles, Commander, United States Public Health Service, Commissioned Corps
Benjamin Bluml, executive director and senior vice president, Research and Innovation, American Pharmacists Association Foundation
Christopher Palombo, board member, Charitable Pharmacies of America
Corey Coleman, vice president, Health Equity and Strategic Partnerships, OptumRx
Dima M Qato, associate professor and senior fellow, Schaeffer Center for Health Policy and Economics, Mann School of Pharmacy at the University of Southern California (USC)
Dixie Leikach, managing network facilitator, Community Pharmacy Enhanced Services Network Maryland
Donney John, executive director, NOVA ScriptsCentral
Douglas Hoey, chief executive officer, National Community Pharmacists Association
Emmeline Paintsil, director of professional affairs, Iowa Pharmacy Association
Jacinda Abdul-Mutakabbir, assistant professor of Clinical Pharmacy, University of Southern California, Skaggs School of Pharmacy and Pharmaceutical Sciences and the Division of the Black Diaspora and African American Studies
Jake Galdo, managing network facilitator, Community Pharmacy Enhanced Services Networks Health Equity; and co-founder and chief executive officer, Seguridad, Inc.
Kate Gainer, executive vice president and chief executive officer, Iowa Pharmacy Association
Lindsey Ludwig, executive director, Community Pharmacy Enhanced Services Network Iowa
Lisa Hines, chief quality and innovation Officer, Pharmacy Quality Alliance
Lisa Yu, director, Customer Marketing and Value Based Care, The Janssen Pharmaceutical Companies of Johnson & Johnson
Magaly Rodriguez de Bittner, professor, the University of Maryland School of Pharmacy
Melissa Castora-Binkley, senior director, Research, Pharmacy Quality Alliance
Parisa Vatanka, co-founder and chief executive officer, Digital Health
Rachel Harrington, senior research scientist, National Committee for Quality Assurance
Rajul Gandhi, population health clinical director and dyad, Carle Health; and chief clinical officer, Stratum Med, Inc.
Rina Shah, senior vice president, Pharmacy of the Future & Transformation, Walgreen Co.
Roger J. Paganelli, pharmacist and co-owner, Mt. Carmel Pharmacy; and luminary/lead network facilitator, Community Pharmacy Enhanced Services Network New York City
Sandra Leal, vice president, Pharmacy Practice Innovation and Advocacy, CVS Pharmacy
Seth B. Gazes, system director of strategy and planning, Geisinger pharmacy
Sherrise Trotz, founder and chief executive officer, Pink Sage Inc.; and former vice president, Operations Chicagoland Region, Walgreens
Susan Cantrell, chief executive officer, Academy of Managed Care Pharmacies
Tripp Logan, vice president, SEMO Rx Pharmacies and Services; and lead luminary, Community Pharmacy Enhanced Services Networks Health Equity
We express our thanks to other respondents we interviewed for this project who chose to remain anonymous or whose permission to be credited was not received in time for this publication.
Cover image by: Alexis Werbeck

{kind=link}