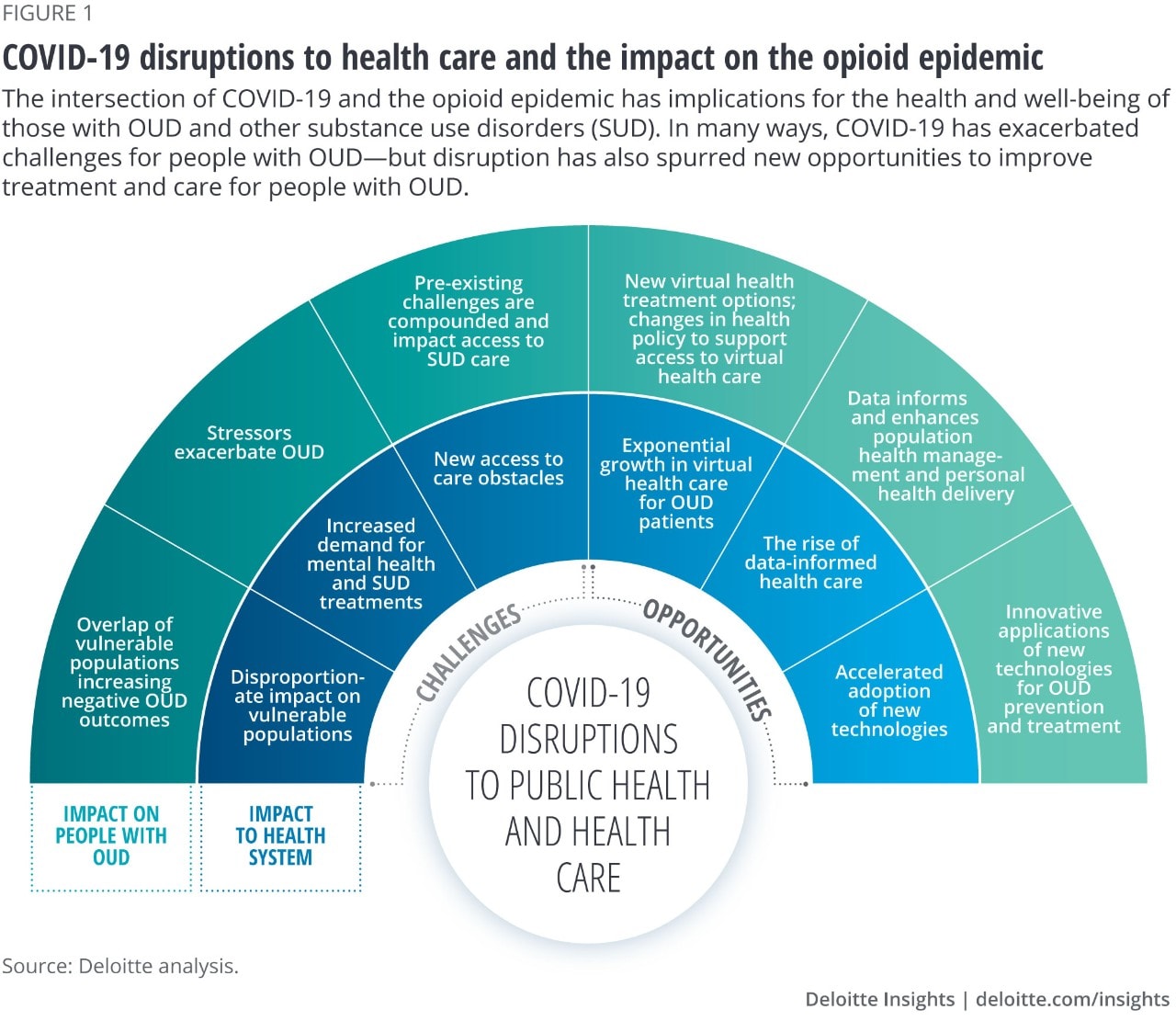
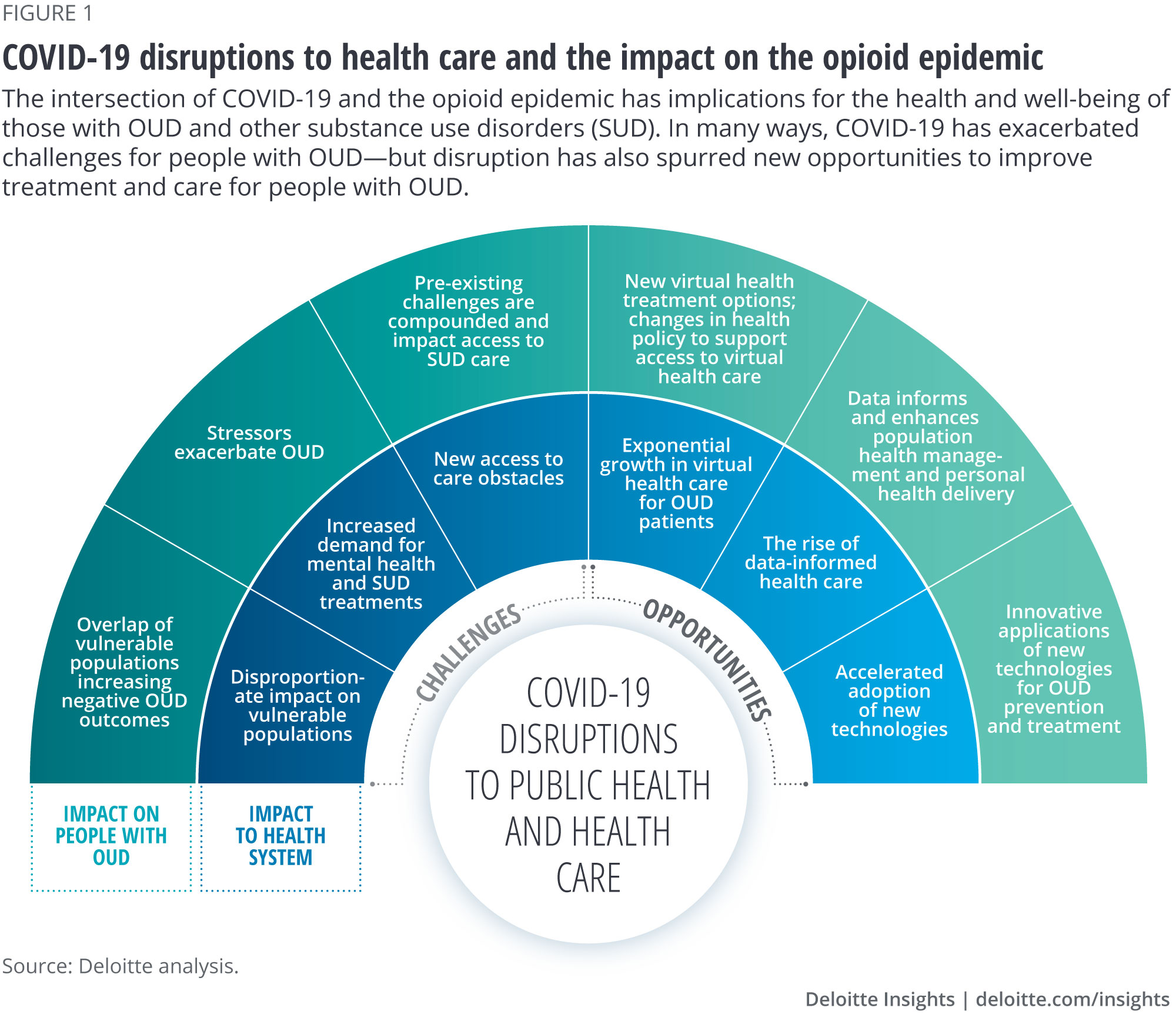
New access to health care obstacles
Even as stressors related to the pandemic have exacerbated mental health and SUD challenges, the pandemic has disrupted health care operations, which are necessary to address those challenges. These disruptions have introduced new issues with treatment of people with SUD with devastating consequences. In certain areas, in-person recovery programs have been halted or limited to maintain social distancing.12 For some patients, required medical appointments to refill treatment prescriptions (e.g., monthly injections of medication to support OUD recovery) were delayed. In at least one documented case, this led to withdrawal, relapse, and death as a result of overdose.13 Some of these social distancing mandates have since been relaxed, enabling prescribers to provide additional weeks’ worth of medication to avoid interruptions in care.14 Access to other services, such as syringe services programs and other harm-reduction resources, have undergone operational disruptions as well.15 Finally, across health care, many patients are delaying treatment—including avoiding emergency room visits for critical care needs (which could include opioid overdose)—due to fear of contracting COVID-19.16 In addition to new obstacles generated by the pandemic, there are existing challenges for people with SUD who try to access care. For example, gaps in broadband infrastructure to support virtual medical visits, absence of transportation, and lack of health insurance are all increasingly difficult to overcome in combination with new obstacles created by the pandemic.
Opportunities for innovation
While the COVID-19 pandemic will continue to exacerbate many existing issues related to the opioid epidemic, it could also fuel progress toward improving prevention and treatment of OUD. The pandemic continues to provide opportunities to scale up existing strategies and develop completely new strategies to address OUD, which may leave a lasting impact even after COVID-19 subsides.
Exponential growth in virtual health care for OUD patients
Creative policymaking for virtual health during COVID-19 should be applied to other public health challenges, such as the opioid crisis.
Virtual health—defined as a variety of “at-a-distance” interactions that further the care, health, and well-being of health care customers in a connected, coordinated manner17—provides new treatment approaches and expands access to care for OUD. Health care delivery at a distance will likely continue to grow as the United States navigates COVID-19 outbreaks and works to minimize in-person interactions.
As a result of COVID-19, the federal government implemented sweeping regulatory waivers and flexibilities to enhance access to virtual health services such as telemedicine. For example, while 76% of hospitals had fully implemented telemedicine by 2017,18 its use has increased manifold during the COVID-19 pandemic. Prior to the pandemic, about 13,000 fee-for-service (FFS) Medicare beneficiaries used telemedicine in a week; in April 2020, this number grew to almost 1.7 million users a week.19 This shift, facilitated by an influx of regulatory flexibilities, might have accelerated virtual health by a decade.
The pandemic’s impact on virtual health has already altered the way many people being treated for OUD receive care and improved access to treatment for SUD. Medication-assisted treatment (MAT), sometimes also known as medication for opioid use disorder (MOUD), involves the combination of behavioral therapy with the use of methadone, buprenorphine, or naltrexone to address neurological components of SUD (e.g., blocking withdrawal symptoms). Prior to COVID-19, issues such as provider shortages, strict federal and state care delivery policies, transportation challenges, and stigma created challenges to MOUD/MAT access, especially in rural areas.20













{kind=link}