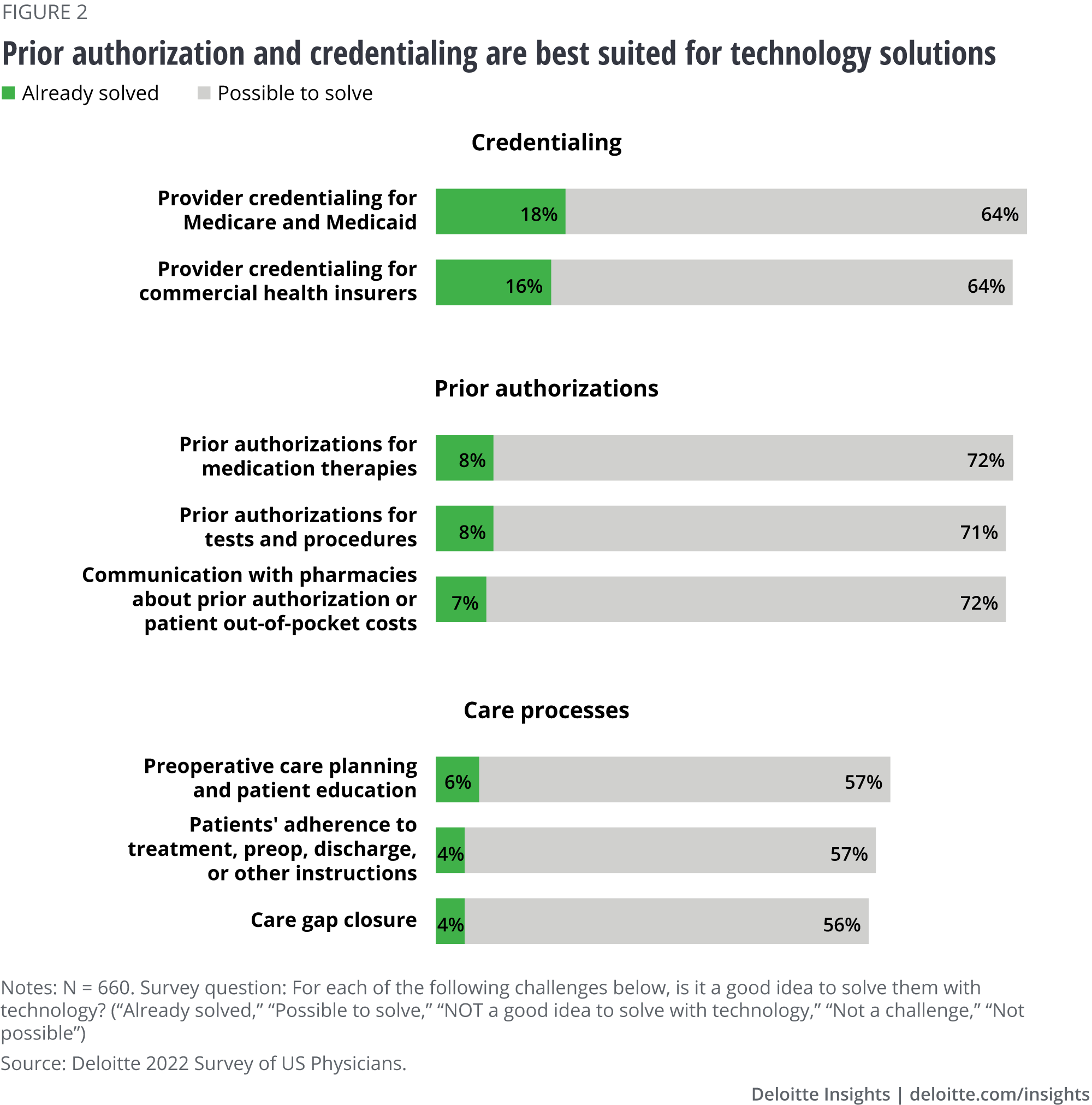
The severe shortage of health care workers alongside greater use of contract labor during the pandemic may be responsible for the 9 percentage point reduction (from 2020 to 2022) in the amount of work physicians say is possible to delegate. As experienced clinicians left the profession or switched to contract assignments, many organizations faced a loss of institutional knowledge and experience. As a result, it’s harder for the clinicians who stayed to confidently delegate and, in some instances, find somebody to delegate to.9
When we look at the responses by care setting and employment, there is little difference in the amount of work physicians estimate can be performed in nontraditional settings. Also, independent and employed physicians in outpatient settings have a similar notion of how much of their work can be automated or delegated (about 20%). However, independent physicians practicing in inpatient settings say a smaller share of their work can be automated or delegated (about 13%) than their employed counterparts (25%).
Physicians say a smaller share of clinical care (than share of total work) can be automated, delegated, or performed in nontraditional settings (figure 3). Nonsurgical specialists say a higher proportion of clinical care (29%) can be performed elsewhere than primary care physicians (23%) and surgical specialists (18%).
Analysis of responses based on the use of comprehensive care teams points to interesting possibilities.10 Physicians who routinely use comprehensive care teams estimate that a bigger share of the clinical care they personally provide can be automated, delegated, or shifted to nontraditional sites, whereas this isn’t consistently the case for total work. Perhaps, access to a team of experts spanning multiple disciplines gives them the confidence that clinical work can be done well even if they are not the ones doing it. Our data on the use of care teams also shows that when comprehensive care teams are used, physicians say the teams are highly effective and team members largely operate at the top of their license.
Building solutions that take the burden off physicians
Opportunities abound to alleviate the physician burden through a combination of technology, delegation, shifting work to nontraditional settings, and other tools. While some physicians express skepticism about the ability of technology to solve problems, others are optimistic. We believe this is especially true if there is an honest discussion about what technology can and cannot accomplish and what new issues or unintended consequences may arise.
To make meaningful improvements to physician workflow, health systems and solution developers should have a nuanced and precise understanding of physicians’ needs and build solutions that not only are useful and easy to use but also restore joy in the practice of medicine.
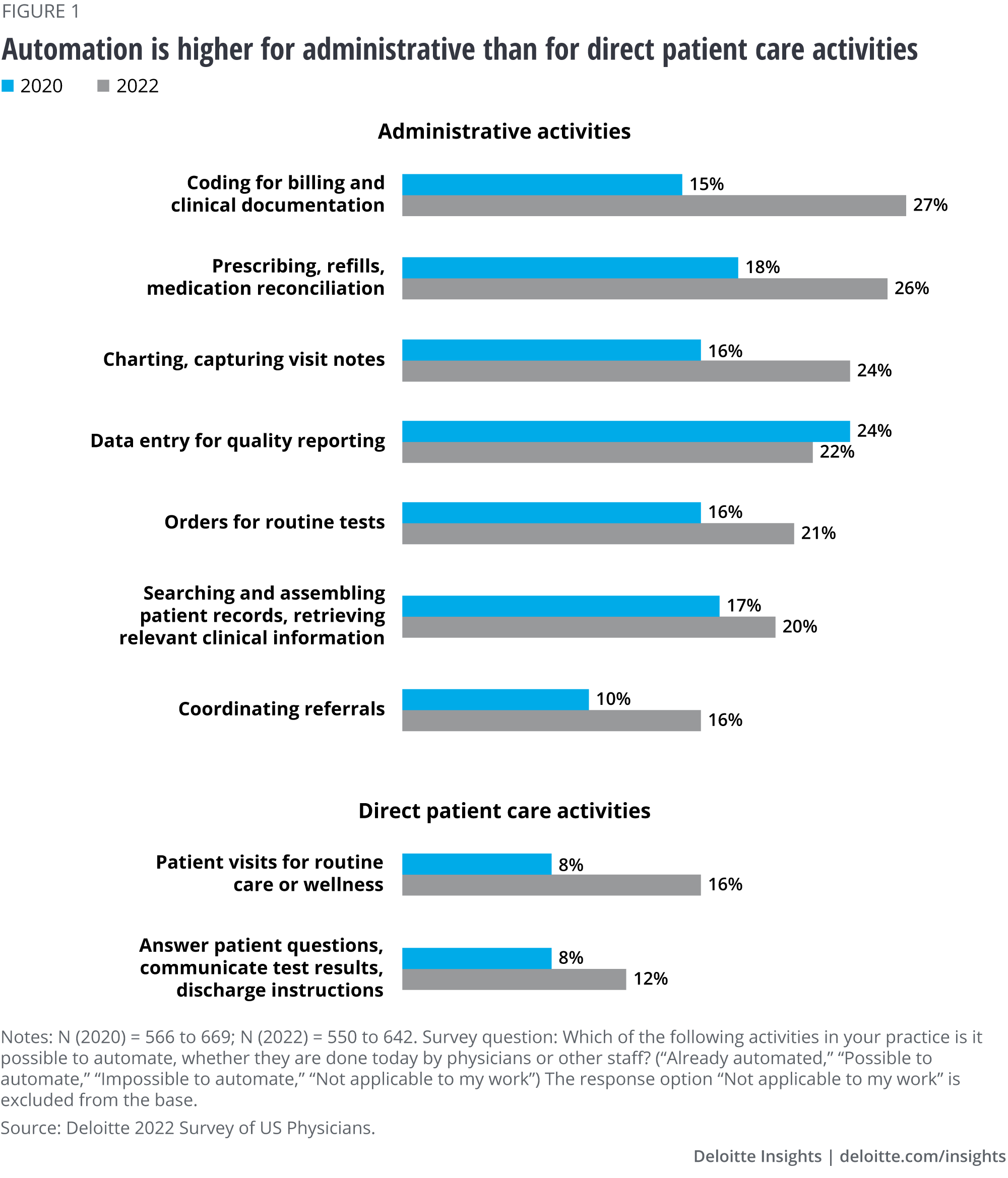
- Optimize prior authorizations, especially in outpatient clinics. If PA functionality already exists inside the EHR and is sufficiently robust, health systems should ensure it is turned on and the connections to Surescripts and other prescription adjudication and payer platforms are enabled and accurate. Efforts should be put in place to optimize this functionality for the practice workflow and train the staff on how to use it effectively.
- Learn the specific pain points physicians who work in your organization or network face. What’s challenging for some physicians might not be an issue for others. These differences are informed by specialty, practice setting, existing workflows, and even years in practice. Organizations should make sure they understand these dynamics among their own clinical staff and their network providers.
- Conduct needs assessment and identify process improvement opportunities using EHR analytics, ethnographic observations, time use studies, and traditional market research techniques.
- Perform an audit of discreet tasks performed by clinicians and staff. Work with stakeholders to assess the clinical, quality, business, and compliance needs for each existing activity, and look for opportunities to eliminate or combine activities or extract from other sources the data they aim to generate.
- Understand how discrete tasks and processes are connected, where one process ends and the other begins. Often, automating or streamlining a portion of a process doesn’t create savings or efficiencies until the entire process is changed.
- Conduct user experience research early in the development process when there is still flexibility to make changes based on user input. Perform ongoing usability testing as new features are added and processes evolve.
- Implement change management to support individuals, teams, and departments in adopting and adapting to the new processes.11 The transition to new processes should be transparent, explainable, and respectful of staff’s time.
- Establish operational and governance processes. Specifically:
- Adopt a standard and transparent approach to evaluating and prioritizing use cases for investments. Metrics around value and implementation complexity can be a starting point. For more information, see “Value and complexity can be used to prioritize use cases for workflow redesign.”
- Build a governance structure to bring the discipline and consistent methodology to opportunity identification, evaluation, execution, and KPI measurement.
- Establish a center of excellence that performs the governance oversight and acts as a shared resource to convene experts in technology and process improvement, evaluate opportunities, and drive the implementation.
By instituting the right combination of technology and other solutions, health care organizations can help simplify the physician workflow—and reap the benefits. The goal is to reduce the cognitive burden on physicians, give them more time to spend with patients, and help ensure that clinical value isn’t sacrificed.
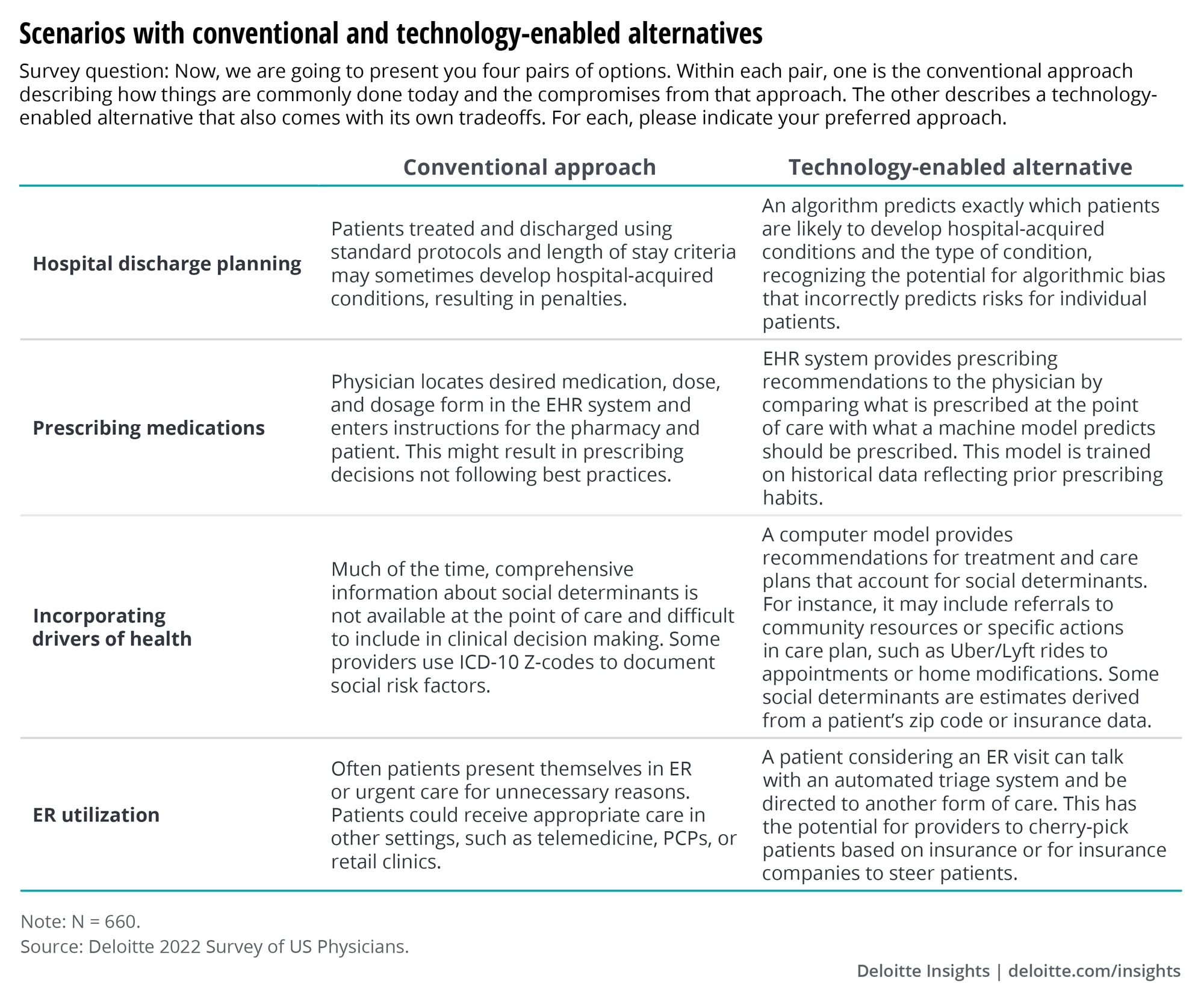
Appendix 1. Scenario exercise from the survey
The respondents were presented with a conventional approach and a technology-enabled alternative that came with new tradeoffs. Respondents indicated their preferred approach for each of the four scenarios.
























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}