Article
Thoughts on healthcare management in an epidemic
Throughout the history of humankind, there have been several large outbreaks of infectious diseases, and the death toll of these diseases is comparable to numbers of lives lost in wars. Within the 20 years of the 21st century, there have been numbers of large epidemics, such as SARS, H7N9, Zika, Ebola, and now COVID-19. The current fight against the novel coronavirus is not only a pressure test of China's overall medical system, but also a severe challenge to each hospital nationwide, especially in public health emergency identification speed, emergency management capacity, and the ability to reserve and distribute supplies.
Response to epidemic requires the participation of an entire society. Deloitte believes that, as government agencies, organizations should think about how to improve capacity and efficiency of early warning and scope control for infectious disease. Hospitals and other primary medical institutions could try to strengthen their comprehensive management ability, including emergency management, to react and implement "wartime measures" promptly, while taking care of other patients' needs and safety. Corporations may consider to continue focusing on employees' health condition during the outbreak, provide mental supports when necessary and perform pointed employee health management activities after the crisis. Meanwhile, the topic of making greater use of digital technology and advanced management methods to raise the level of people management, supply chain management, and telemedicine capability in healthcare institutions deserves further exploration for all stakeholders in this society.
For the present and the future, Deloitte suggests stakeholders, especially in the healthcare sector, pay particular attention to the following matters:
Improve emergency management systems in healthcare institutions:
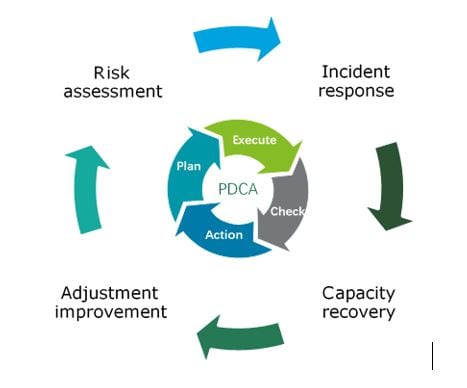
The purpose of establishing an emergency management system in healthcare is to prevent and react to emergencies effectively, as well as to avoid, minimize and mitigate the negative impact of the incident, through cross-functional collaboration. The goal of the management system is to design and create a fast and flexible organization based on emergency management objectives, clarify its responsibilities and powers, and coordinate internal resources, to ensure operational effectiveness and efficiency under emergency.
The design of the management system usually incorporates four key phases: risk assessment, incident response, capacity recovery, and adjustment and improvement:
- Risk assessment:
- Perform operation risk assessment regularly; based on the assessment result and the characteristics and requirements of public emergency rescue and the prevention of public health emergency, establish a lead group for emergency response, formulate contingency plans for preparedness and response, conduct regular trainings and exercises to strengthen staff flexibility and familiarity of the process, and evaluate process validity of the contingency plan to make continuous improvements.
- Anticipate and prepare essential equipment and materials for emergency response, based on analysis of its local population, environment, medical resources and other factors, and establish channels that can assist in the response and recovery of an emergency.
- Participate in a joint assessment with other local medical institutions and members of the same hospital alliance, to identify supporting capacity of the local healthcare system, including but not limited to skilled healthcare professionals, medical supplies and medical equipment, in response to outbreak incidents.
- Utilize risk analysis tools – Hazard and Vulnerability Assessment (HVA): to analyze the probability of risk occurrence, hospital preparedness, to evaluate the value and impact of each risk to the hospital, and to design management plans and exercise frequency in accordance to prioritized risks.
- Degree of risk damage = Probability of risk occurrence x Risk severity
- Steps in conducting HVA:
- form a collaborative planning team – identify hazards – review historical data – calculate probability – calculate impacts – prioritize risks – calculate preparedness – develop courses of action
- Incident response:
- Initiate emergency plans, implement standard procedures, such as reporting, directing and other cross-functional collaborations. Pay special attention to the emotional and spiritual states of patients' family and medical staffs, to provide timely support and protection.
- Assess the institution's coping capability, if identified as inadequate, reach out to other local medical institutions and/or its alliance for coordination immediately.
- Provide ongoing communication with local emergency management agencies and other authorities, to coordinate and achieve quick response and to support authorities' decision making process for public service, such as traffic control, diversion of affected personnel, supply allocations, etc. thereby preventing the crisis from spreading and minimizing its impact.
- Ensure an open communication channel for all information and reports, encourage healthcare professionals to report healthcare incident as soon as it is determined reportable, and adjust the internal approval process if necessary, making sure the voice of a "whistleblower" can be heard at all times.
- Capacity recovery:
Carry out recovery work, such as environmental cleanups, equipment maintenance, staff reorganization, resource reallocation, etc. promptly, once the incident enters a phase of significant moderation.
Meanwhile, conducting a recovery assessment and formulate corresponding plans are necessary for healthcare institutions. It enables organizations to identify and prioritize essential healthcare assets and services to maintain their operation and return to normalcy as early as possible.
- Adjustment and improvements:
Review the occurrence and the measurements taken in response to the incident and propose improvement countermeasures. With an analysis of the cause and an assessment of its threat level, develop and implement preventative measures and establish a mitigation system to reduce the probability and impact of future crises.
Many countries have established sophisticated emergency management systems that worth learning. Such systems are designed based on the principles of unified leadership, comprehensive coordination, classify to management, and hierarchical control. They cover the entire disaster cycle, including the preparation, the break, the recovery and the mitigation, strengthening the systematization, institutionalization, and standardization of the emergency response mechanisms. Most Chinese medical institutions still need to enhance their top-level design, classification management, standardization and other areas. Although emergency management often sets a comprehensive plan and process, to reinforce its operability, regular training and drills are essential.
Upgrade level of protection for healthcare professionals and patients in emergencies:
During an outbreak, healthcare institutions need to treat patients with extra cautions, especially patients with fever. These patients should be transferred immediately to the fever clinic and take into a virus identification process. However, because hospitals treat not only fever patients, but also patients with other illness, such as chronic diseases which require regular hospital revisits minimizing cross-infection risk to protect patients, patient families, and medical staffs becomes a critical task. According to the evaluation criteria of China's as well as international hospital accreditation standards, medical institutions may take the following measures to avoid preventable losses from cross-infection and to protect the health and safety of their patients and staffs:
- Enhance access control:
As access controls are now exercised in residential areas, healthcare institutions may spend more effort to manage hospital occupancy and access ways, limit passages and attendants, encourage patients to postpone non-urgent examinations, prohibit unauthorized discharges, and monitor people's dynamics, thus performing valid control measures. - Upgrade hospital infection control:
The upgrade of infection control standards may break into two areas – work path management and disinfection regulations.
- Work path management: rearrange work path during the emergency, enforce access control at all open passages, and provide temperature monitoring, mask-wearing requirements and preliminary pre-examination for all access personnel. For high-risk groups, set up a separate passageway to avoid infection risk during transmission.
- Disinfection regulations: in addition to the requirement of a thorough execution of hand hygiene for medical staffs, there is also a need to strengthen environmental hygiene, especially for areas where patients and visitors may touch, such as escalators grips, elevator buttons, handrails, waiting-room bench, etc. Apart from the existing rules in infection control, medical institutions also need to consider reducing the risk of exposure for medical professionals.
Establishing a sustainable supply chain programme:
In the course of outbreak prevention and control, different types of hospitals may face problems within the preparation and security of medical supplies:
- Public hospitals:
Public hospitals that are designated as medical institutions for epidemic prevention and control may face shortages of urgently needed medical supplies due to insufficient early estimates of material demand and the inability of upstream supply chains to respond promptly to their needs.
- Social medical institutions:
Although many social medical institutions were not named in the first batch of epidemic prevention and control hospitals, due to their locations and other factors, they could now be hosting many infected patients. If they have not been given government priority, they may face pressure to procure from unqualified suppliers of high-priced medical supplies.
To respond effectively to an outbreak and ensure sustained day-to-day operations, Deloitte suggests medical institutions take the following material security measures:
- Establish inventory warning system:
- Establish a model for daily operation and measurement of medical needs at different risk levels.
- Give full consideration to storage costs, efficiency management, shortage risks and other factors, and set up inventory early warning indicators.
- Build sustainable supplier relationships:
- Taking into account the interests of all parties, seek common goals in product quality, cost, and response time in the upstream and downstream of the supply chain.
- Clarify suppliers' responsibility in terms of the scope and timeliness of material provision in non-emergency periods through a contract or memorandum.
- Sort end-to-end supply process:
- Sort out the supply process, end-to-end, from the need for materials in clinical departments to measures that improve the efficiency of their planning and supply.
- Private medical institutions should maintain timely communication with government departments and establish feedback channels for requests for materials.
- Establish a joint reserve allocation system:
- Clarify the functions of medical materials deployment in emergency situations, establish a transparent supply chain information system, and set priorities for material deployment.
- Qualified private medical groups should carry out centralized procurement and establish joint reserves of materials to reduce procurement and storage costs.
- Identify hospitals or departments with over-allocation of materials and promptly adjust supply plan configurations.
- Take advantage of digitalization to improve the entire supply chain system, including hospital order placement – supplier acceptance – logistics dispatching – authority monitoring, to ensure its transparency and continuity.
Establishment and deployment of dynamic talent management at medical institutions:
In response to the outbreak, the state has led the construction of hospitals, including Huoshenshan Hospital, to treat confirmed new coronavirus confirmed patients, but in terms of medical service personnel, although more than 10,000 medical workers have come to the aid of Hubei province, there is still a shortfall of more than 2,000 medical staffs. There are three possible reasons for this shortfall: the number of available medical personnel is chronically inadequate; the epidemic's occurrence during Spring Festival meant a certain amount of medical personnel had returned home and were unable to return to work as scheduled; and the rapid spread of the epidemic in Hubei had not been anticipated. Medical staff from across China were sent to help in Wuhan, but it is also important to consider whether the medical institutions at which they usually worked suffered shortages of personnel due to the departure of their support staff, and therefore whether there is room for optimization of how medical institutions manage and deploy talent. The following points warrant consideration:
- Sound talent record keeping and file management:
Sound overall management of personnel files, and improving how medical staff's professional and clinical experience, and other information, is updated, not only ensures that when a sudden situation occurs, the most suitable existing personnel and candidates can be found quickly, but also can determine when there will be a staff shortage. - Staying on top of employee dynamics:
In addition to being concerned about the dynamics of serving staff, retired employees should also be included in file management because of their familiarity with a hospital's working model and possible use as alternative staff during an emergency. - Establish talent matching model for healthcare workers:
Establish a talent matching model covering different types of medical care, including normal state and emergency state requirements, which includes the talent requirements of different jobs and organizational structure requirements. When there is strong demand for medical staff, some work can be transferred to personnel who do not need a medical background, and some can be given to personnel with relevant care backgrounds. Medical institutions need to pay more attention to the construction of talent hierarchies, and establish necessary training and assessment for reserve personnel.
Accelerating the development of telemedicine and wearables:
During the outbreak, several internet-based medical institutions have been offering online consultations screening for the common cold and new coronavirus pneumonia, relieving pressure on offline medical services and reducing cross-infection, but also allowing more people to get used to the internet medicine experience. Some preliminary management standards are governing online healthcare, including the Internet Hospital Management Measures, Internet Diagnostic and Therapeutic Measures and Remote Medical Service Management Code. Although online healthcare has been a critical trend in the medical sector over recent years, its promotion and popularization still face challenges.
- The online clinic segment is still in an explosive growth phase, with companies of various sizes and not enough standard diagnosis and treatment mechanisms to make it popular.
- Internet medical care is still subject to policy restrictions, which means it is unable to replace traditional consultations.
- Except for follow-up consultations for some chronic diseases, online and offline medical services are not yet connected, and how to improve connectivity and achieve a transformation remains challenging.
In the face of these dilemmas, Deloitte suggests:
- Hospitals should promote internet medical services:
Vigorously develop internet medical services, including telemedicine services for patients in an emergency or who are unwilling to, or would struggle to, reach a hospital for treatment, as well as to avoid having mildly ill patients attend hospital. This can also shorten the length of hospital stays and reduce the risk of infection for patients who have to attend a hospital for examinations or to receive the medicine. Staffing of departments dealing with non-communicable diseases can also be adjusted accordingly, doctors can provide online medical services to people at home, and the number of nurses can be reduced to ameliorate the risk of infection. - Wearable devices for people with chronic diseases:
Wearable devices can monitor a user's heart rate, blood pressure, blood oxygen, electrocardiogram data, and send this to a server and APP in real-time. If the data reaches a pre-set threshold, family members and local community health centres can receive equipment alerts to keep abreast of the patient's status. Also, data collected by wearables can be shared to an internet medicine platform and used to support the re-diagnosis of patients with chronic diseases, enabling doctors to adjust medication according to changes in those patients' conditions. - Enhance primary community diagnosis and treatment through telemedicine:
Emergency management systems covering grass-roots communities can be improved through telemedicine and other means, helping to ascertain the actual availability of community medical resources, general practitioners and family doctors, and deal with emergencies concerning residents' health security through a rapid response mechanism. At the same time, telemedicine can improve mechanisms for graded diagnosis and treatment, allowing family doctors to provide residents with offline or online initial consultations, strengthen the integration of medical provision at all levels, and improve the capacity of community healthcare systems.
It is important to note that, since medical devices and technology concern the lives and health of patients, all equipment and networks must be managed and subjected to rigorous disaster tolerance testing that ensures equipment and system operate properly during an emergency.
Designing a comprehensive health management systems for enterprises:
The prevention and control of COVID-19 outbreak are still at a critical stage, yet, according to the central government, many companies and organizations are beginning to resume regular work and production.
After a company resumes work, it needs to consider how to ensure total prevention and control, maintain a safe corporate office environment, determine key elements of the company's health management system, and how to respond to emergencies that might occur. Deloitte suggests:
- Establish an emergency system and risk management team:
Set up an emergency team for outbreak control, create emergency and business recovery plans to minimize the impact of the outbreak on business by ensuring the health and safety of the employees. - Assess employees' health risks and adjust business plans:
Before an epidemic is adequately controlled, an enterprise should, according to its specific characteristics, establish performance measures for remote-working to ensure its regular operation through a flexible office system. The enterprise also should ask employees to conduct a health risk self-assessment based on their medical history and physical condition and require every employee to submit relevant and truthful information. An enterprise can consider screening the health status of returning workers through a health questionnaire, and for staff who must return to work but are assessed as high-risk, consider approaches such as a pre-work check-up to determine whether they should be allowed to enter the company's premises. Management and HR should adjust business plans per employee health risk assessments and medical examination results. - Targeting employee health plans:
An enterprise should take the initiative to establish employee health files and follow-up management, as well as to provide employees with epidemic prevention of personal health training during epidemic prevention and control. It can consider cooperating with insurance companies to launch diversified employee health protection programs and improve the rapid claims process. Also, an enterprise can consider working with medical examination companies to screen for outbreaks, and automatically update employee health files, as well as providing routine annual physical examinations. At the same time, an enterprise could work with health management companies to build a corporate health management platform, set up corporate infirmaries or liaise with community medical institutions to provide convenient medical support to employees through business-community cooperation centred on family doctors, and even personalized healthcare guidance and intervention for employees' families. This can include comprehensive health management services from physical examinations to post-examination medical treatment, thereby providing convenient, timely, and tailored medical support that forms a closed loop of enterprise health management. - "Epidemic Anxiety" control:
The mental health of employees is just as important as their physical health. As individuals, employees are prone to anxiety, depression, stress, complaints, fear of "suspicious diseases", shunning crowds and social situations, job burnout, and other mental health issues. Because of the rapid spread of information, people's ability to sympathize and empathize becomes more vulnerable. An enterprise's HR department should promote its Employee Assistance Program (EAP) to employees in need and provide emotional support and psychological guidance.
Building a national health data platform:
During this epidemic, the real-time sharing of the medical records of suspected and confirmed patients has been challenging. Some patients have left the hospital in panic after visiting the fever clinic or rushed to more developed cities seeking better medical treatment, which made the overall disease prevention and infection control more difficult. Also, due to the Spring Festival travel, and many patients visit the local hospitals with no access to their medical records, making it difficult to provide personalized healthcare. Furthermore, it has been difficult for Centers for Disease Control and Prevention to quickly obtain people's health data for epidemiological analysis and use it to put forward opinions on infectious disease control.
Deloitte believes it will be necessary to speed up the construction of a health data platform covering China's entire population and build a joint database of existing and under construction government and platform hospitals, so residents' health information can be available nationwide and used by the railway, civil aviation, and medical insurance sectors. Also, once these various systems are interconnected, details of patients' treatments can also be quickly shared through the platform. It will enable medical experts to quickly issue diagnosis and treatment plans based on case information from across the country, and doctors in other regions will also be able to refer to a patient's diagnosis and treatment plan to adjust how it deals with similar cases and thereby improve overall treatment efficiency.
The recommendations above are derived from a combination of Deloitte analysis and leading international practices. We believe that through this fight against the ongoing epidemic, China's health system will continue to be optimized and improved.