To understand what steps health systems should take to address the talent emergency, the Deloitte Center for Health Solutions conducted two streams of research to examine the problem from multiple perspectives and identify short- and long-term solutions. From April to June 2022, we interviewed 29 US industry experts, including health system executives responsible for clinician well-being, operations, human resources, and strategy, as well as nursing and medical administrators, scholars, and policy advisors. In August 2022, we surveyed 500 US frontline clinicians who currently or recently practiced in acute and ambulatory settings including, 250 nurses, 170 physicians, and 80 advanced practice providers.
The talent crisis has begun to attract more attention: The Office of the Surgeon General and a few industry groups have issued statements and made appeals to the industry to address burnout among health care workers.1 Developing long-term solutions requires a thorough understanding of the problem—and how it has evolved. Until recently, approaches to improve well-being targeted individual factors such as employee resiliency.2 There is now broad recognition that organizational and systemic factors—work design, culture, workforce supply, and policy—are major contributors to worker burnout, which, in turn, leads to worker shortages.3
To address the underlying drivers that have led to the talent emergency and achieve a long-lasting impact, our research shows that health systems should fundamentally transform the way they deliver care. It's time for the industry to acknowledge that old tools have outlived their usefulness and that we need innovative approaches to how clinicians work, who they work with, and where they work. While redesigning the work should be at the center, these transformation efforts are unlikely to succeed without making ongoing investments in people and rebuilding trust in leadership.
Reimagine care delivery and redesign the work
Chronic burnout is proof that clinicians’ jobs are unsustainable, and the industry cannot continue with the status quo. Yet, our survey data suggests that the status quo is the norm. Surveyed clinicians gave their organizations a grade of “C–” on their efforts to address burnout. The respondents identified many unnecessary and low-value tasks that take time away from patient care, such as those that satisfy administrative requirements (32%) and work that could be done by others or automated (20%), yet they have low expectations of their organizations to innovate.
Most of our interviewed experts, on the other hand, stressed that the path forward involves a complete care model transformation and job redesign. Specifically, they recommend:
- Investing in technology to give time back to workers. For instance, optimizing clinicians’ workflows by getting rid of low-value activities, such as reducing the number of electronic health record (EHR) clicks, can be a quick win. Leveraging automation to reduce time spent on nonclinical work probably takes longer to produce results, whereas new work modalities, such as virtual nursing, that take advantage of remote work possibilities and lessen demands on bedside nurses are longer-term investments.
- Fundamentally rethinking where care is delivered. As more care moves out of hospitals and into outpatient and other alternative sites of care, be smart about staff allocation and preparation and design staff development programs accordingly.
- Redesigning work teams. Implement comprehensive interdisciplinary care teams that take advantage of team members’ strengths, bring in more assistive clinical workers, and allow everybody to operate at the top of their license.
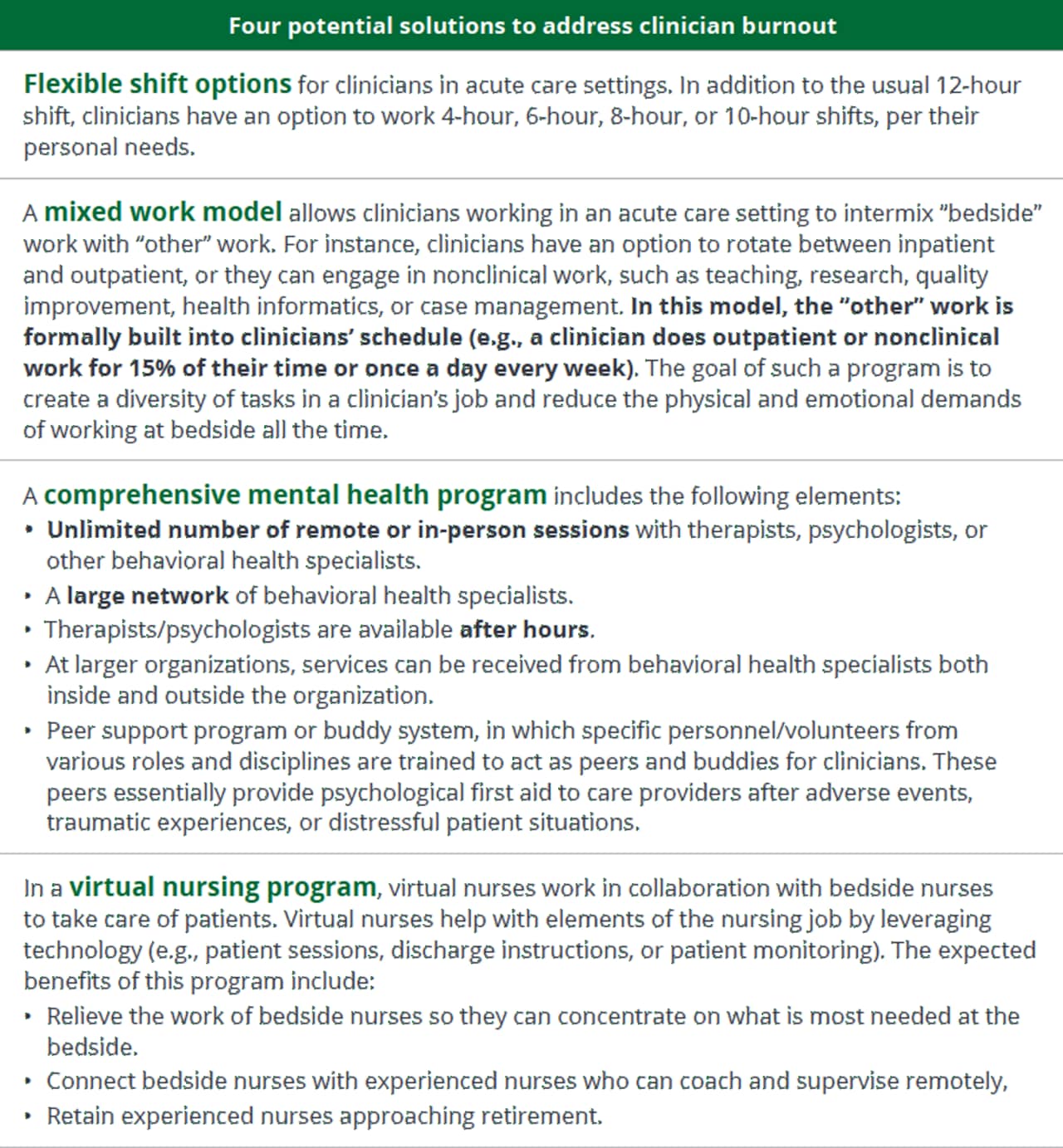
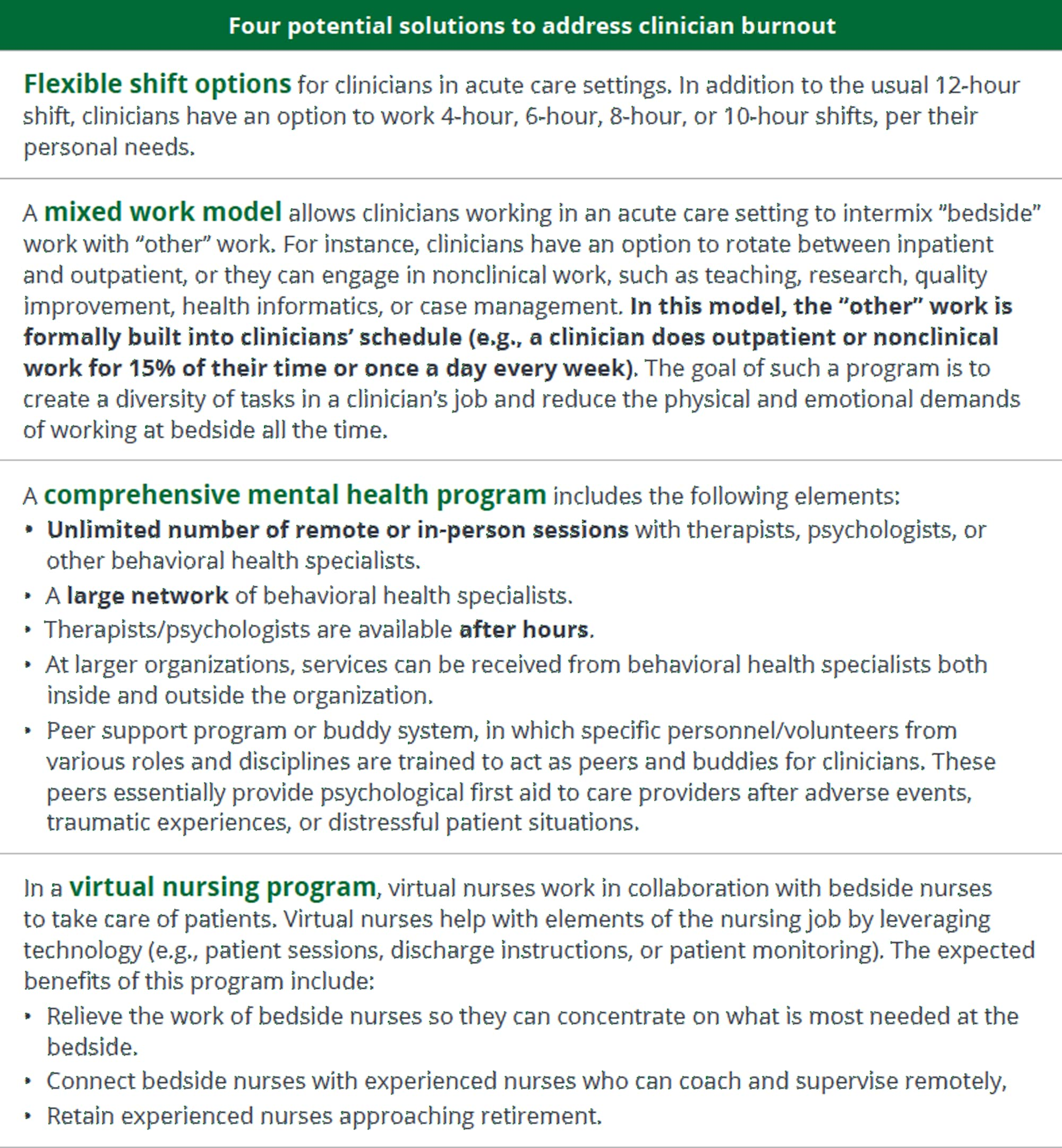
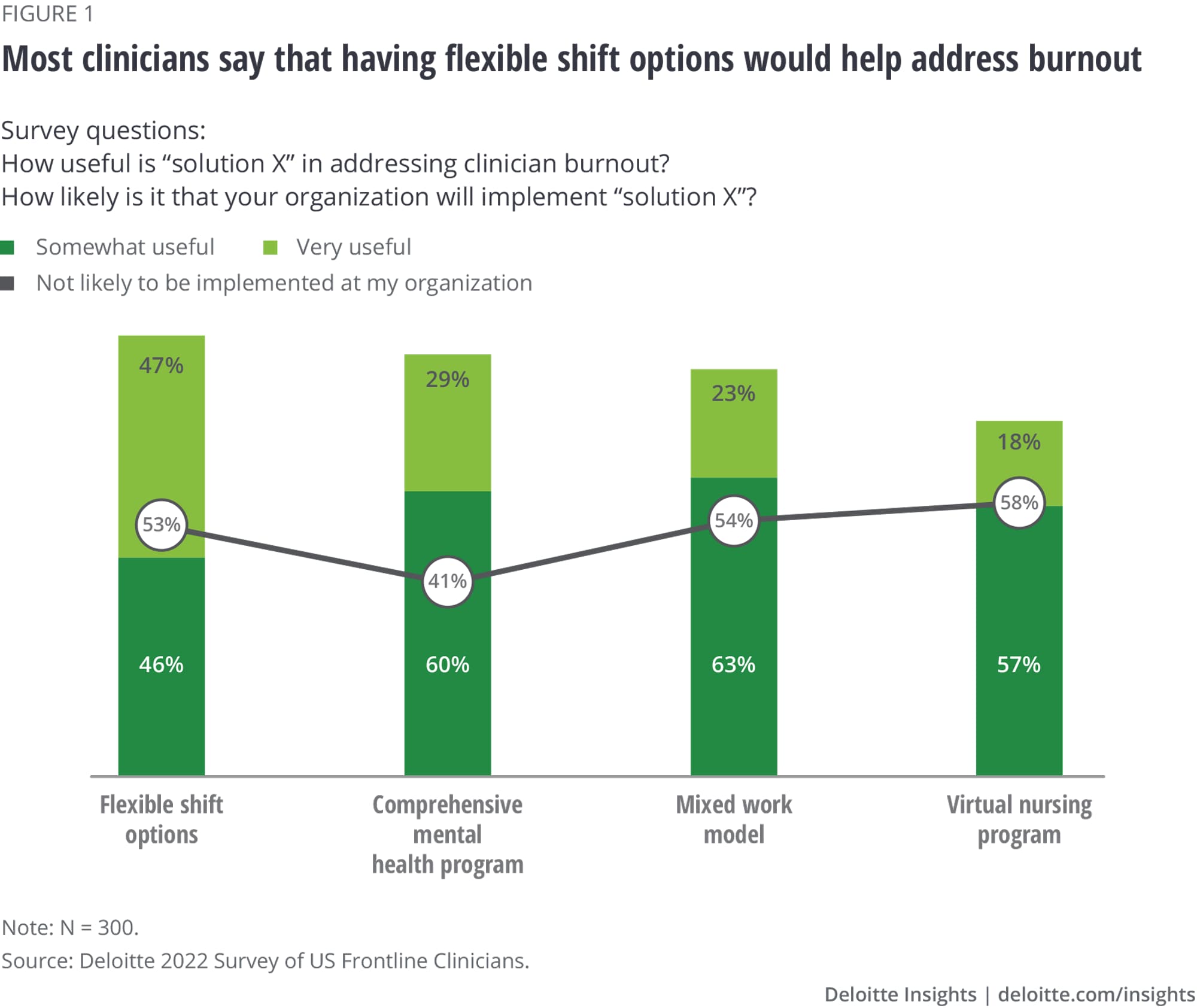
- Injecting flexibility into jobs. The solutions range from flexible schedules and job-sharing to work models that formalize opportunities to intermix bedside work with other types of work.
Invest in your people
Interviewed experts and surveyed clinicians reminded us that because care delivery is a fundamentally human experience, care transformation efforts require investing not only in technology and processes but also in people. Several experts even warned that “we can’t automate our way out of this crisis,” while calls for better staffing were a common refrain in the survey responses.
If satisfaction with compensation and benefits is an indicator of how workers feel about their employers’ investments in their people, our survey results point to a glass-half-full scenario: About half of frontline clinicians are satisfied with their compensation (44%) and benefits (51%). They also say internal career mobility is challenging: Forty-two percent of frontline clinicians find it difficult to change roles inside their organization, one-third (33%) say it isn’t possible, and only 25% say such opportunities are available.
From our interviews, we learned that to attract and retain workers, health care organizations should balance extrinsic and intrinsic rewards, and recognize and accommodate cultural, generational, gender, and life-stage differences. Several forward-thinking organizations spoke of efforts to design opportunities for career advancement and mobility that match employees’ current and future needs.
Interviewees also called for continued investments in workers’ well-being and resources to support self-care, whereas frontline clinicians asked for additional resources to back up those programs—for example, providing enough staff coverage to allow employees to use their paid time off and truly disconnect from work.
Restore trust in organizational leadership
For many organizations, the first step is convincing the leaders to conduct an introspective and honest assessment of their own actions. How well are you caring for your clinicians?
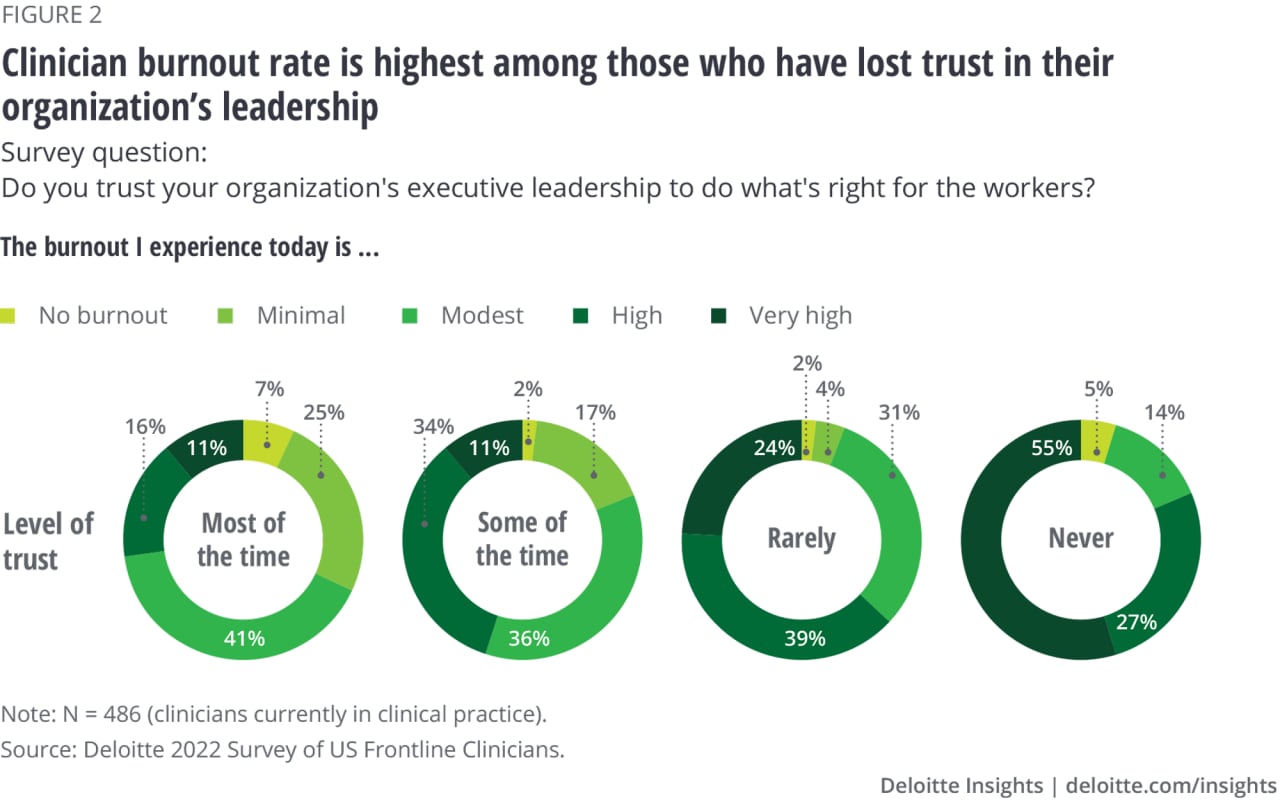
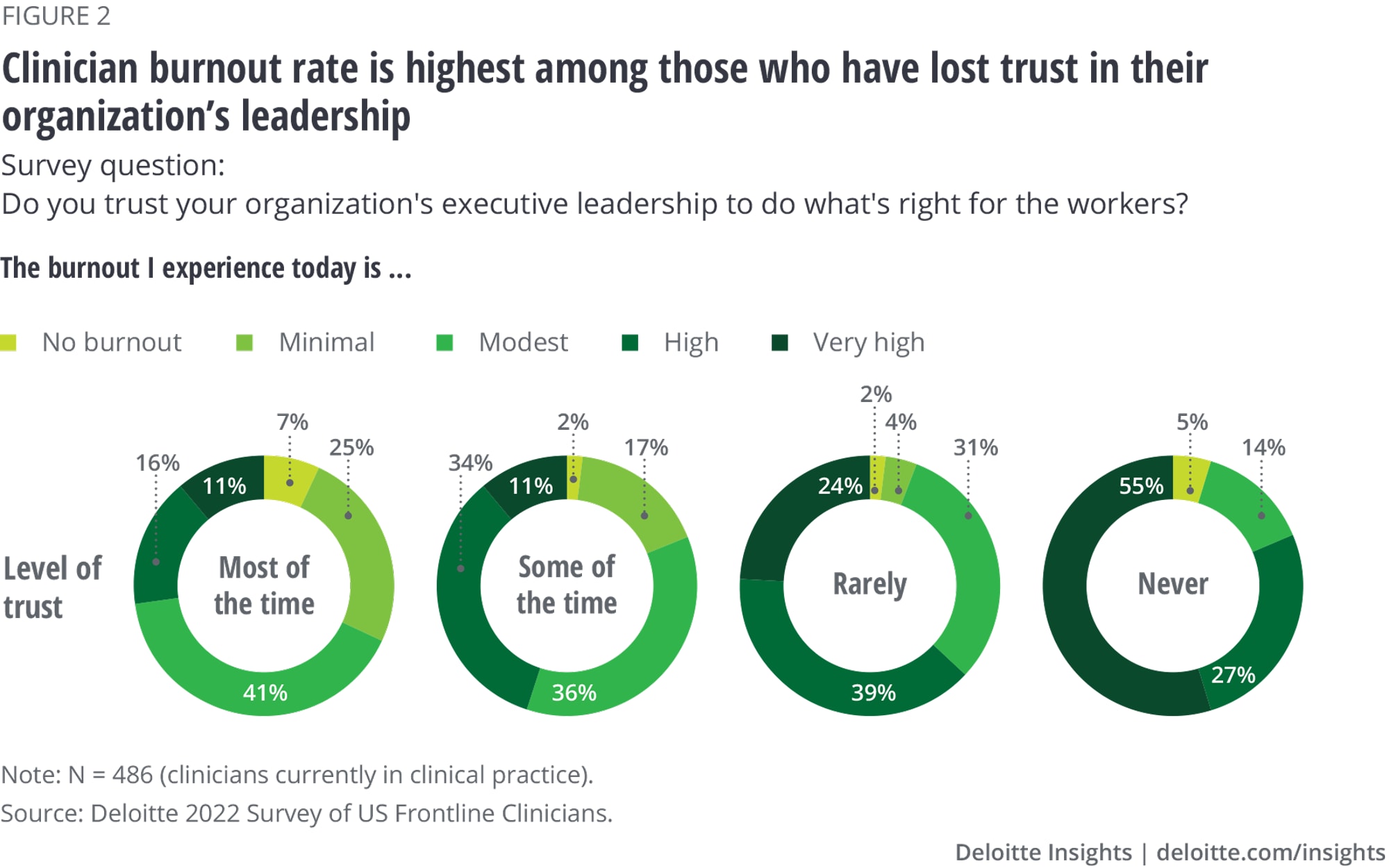
Our survey reveals that fewer than half (45%) of frontline clinicians trust their organization’s leadership to do what’s right for its patients. Even fewer, 23%, trust their leadership to do what’s right for workers. These two types of trust—to do right by patients and to do right by workers—are highly correlated and associated with significantly lower clinician burnout.
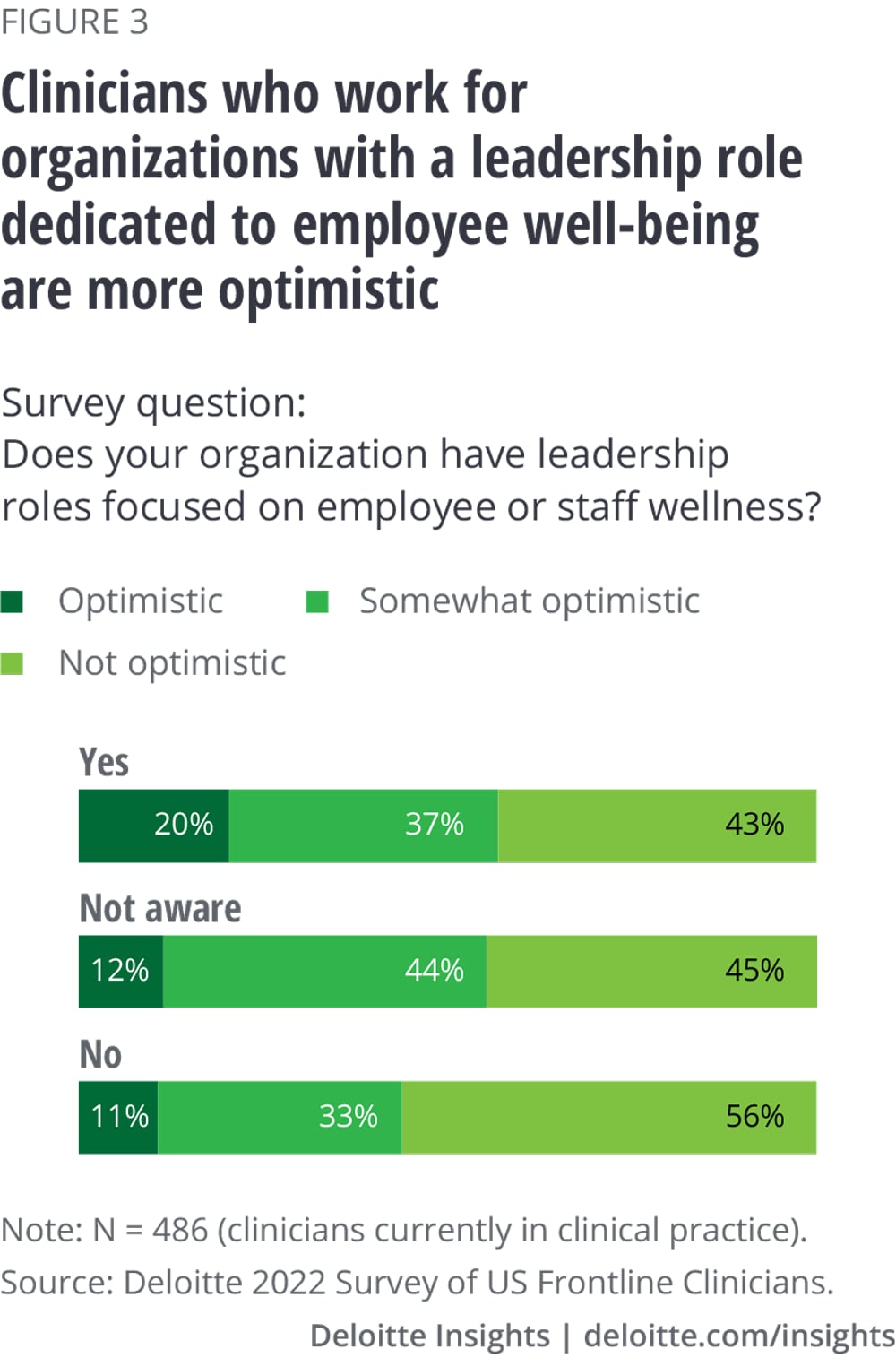
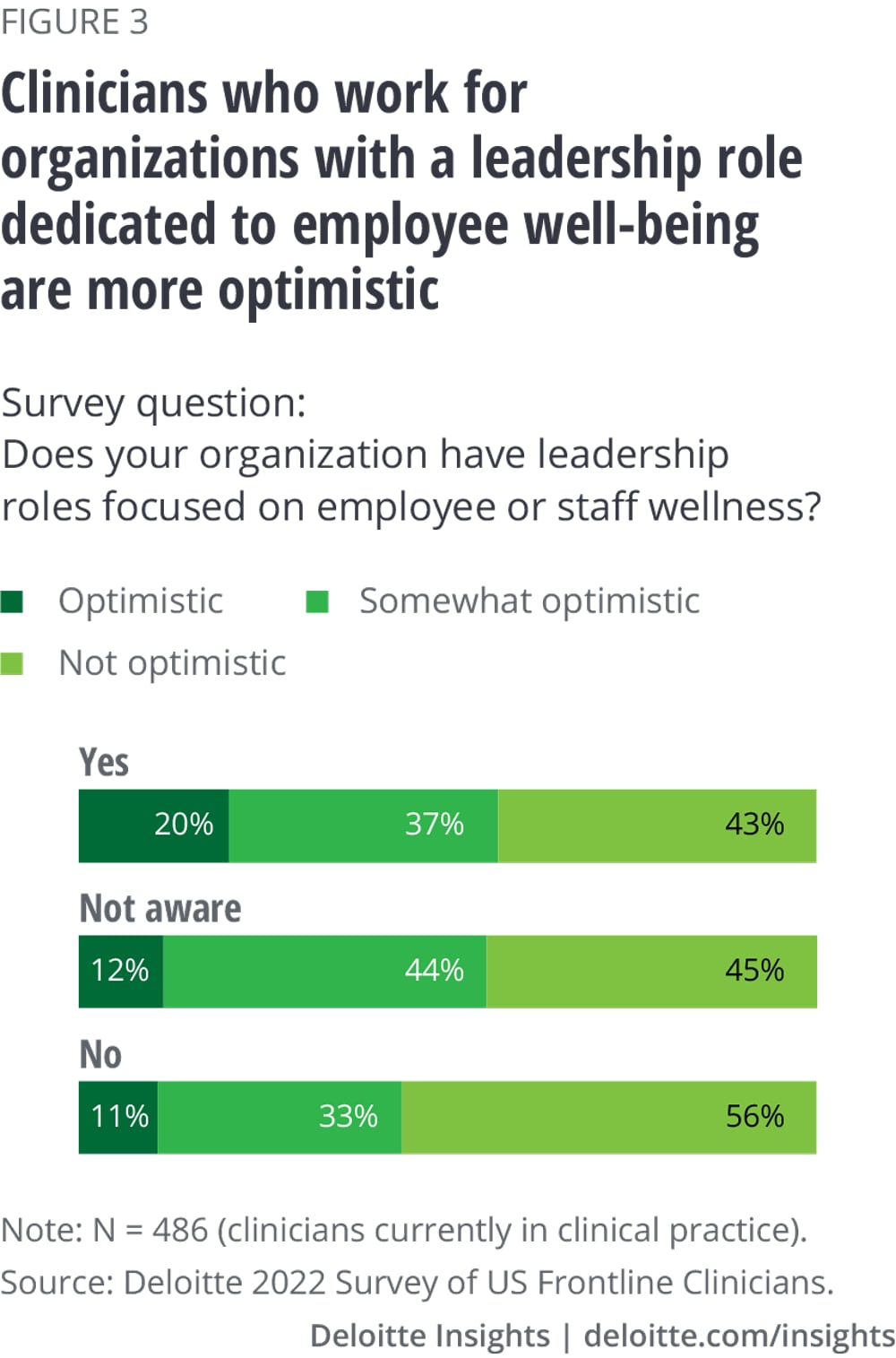
To retain and attract the clinical workforce, health care leaders have a responsibility to rebuild their trust and restore meaning, value, and purpose in their jobs. Listening to frontline workers, recognizing their clinical autonomy, elevating their voice to leadership, and building an inclusive culture are some ways organizations try to achieve this. Holding leaders accountable for worker well-being—by weaving well-being metrics into their compensation and creating leadership positions focused on well-being—can further solidify leadership’s commitment to their workers.
Establish a strong path forward
Frontline clinicians and industry experts are alarmed by the effects clinician shortages have on the quality of care and their ability to deliver on the mission. At the same time, they see this as an opportunity to innovate, learn from each other, and create workplaces and a system of care that can enable patients and clinicians to thrive in the Future of HealthTM.
This mandate to reinvent care delivery comes at a time when margin pressures make it incredibly hard to commit to long-term investments. While hard choices and tradeoffs will be required, perhaps margin improvement programs don’t have to be antithetical to clinician experience. It could be possible to design them in ways that don’t just optimize the costs but also improve population health and enhance the experience of receiving and providing care.
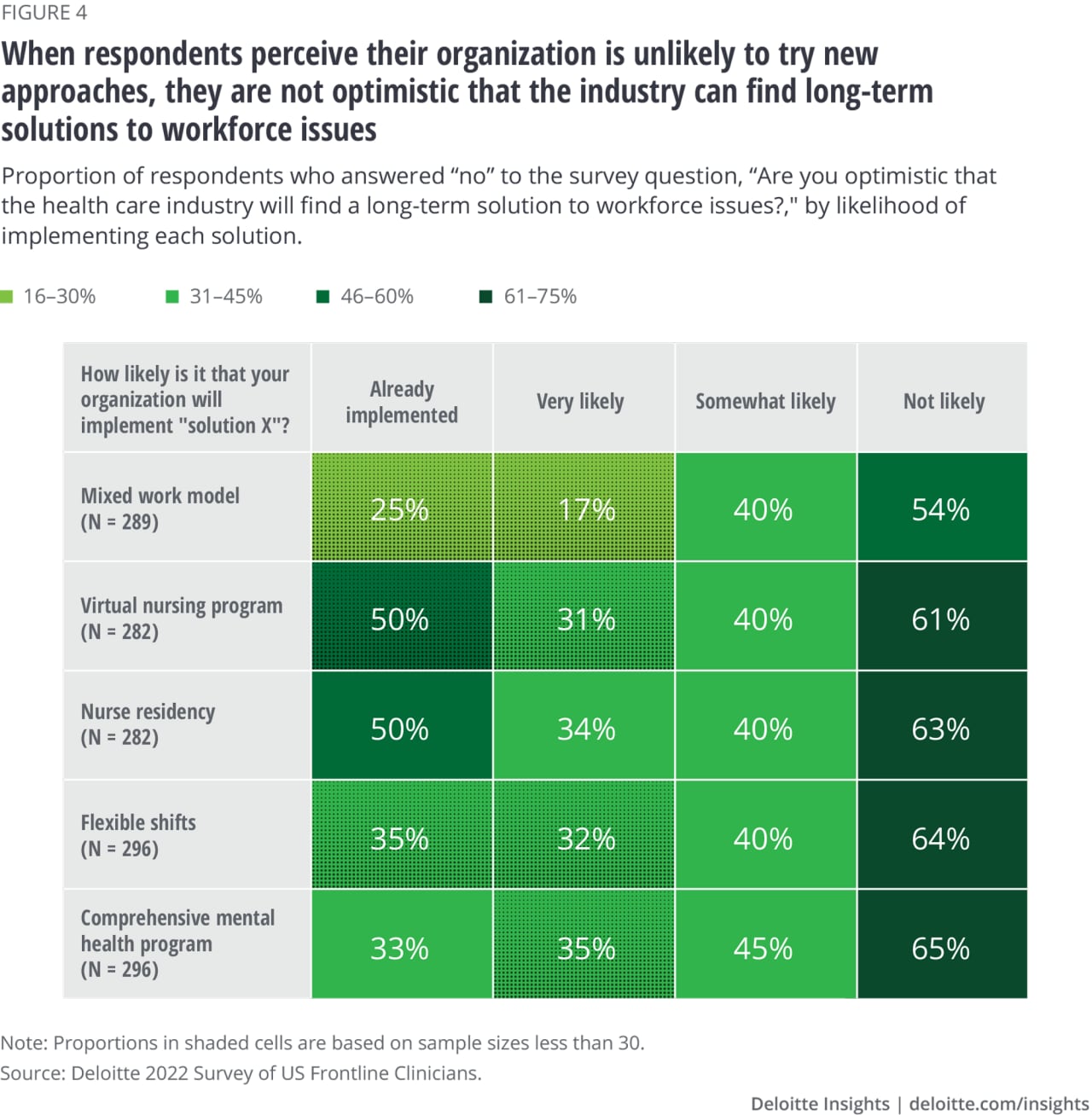
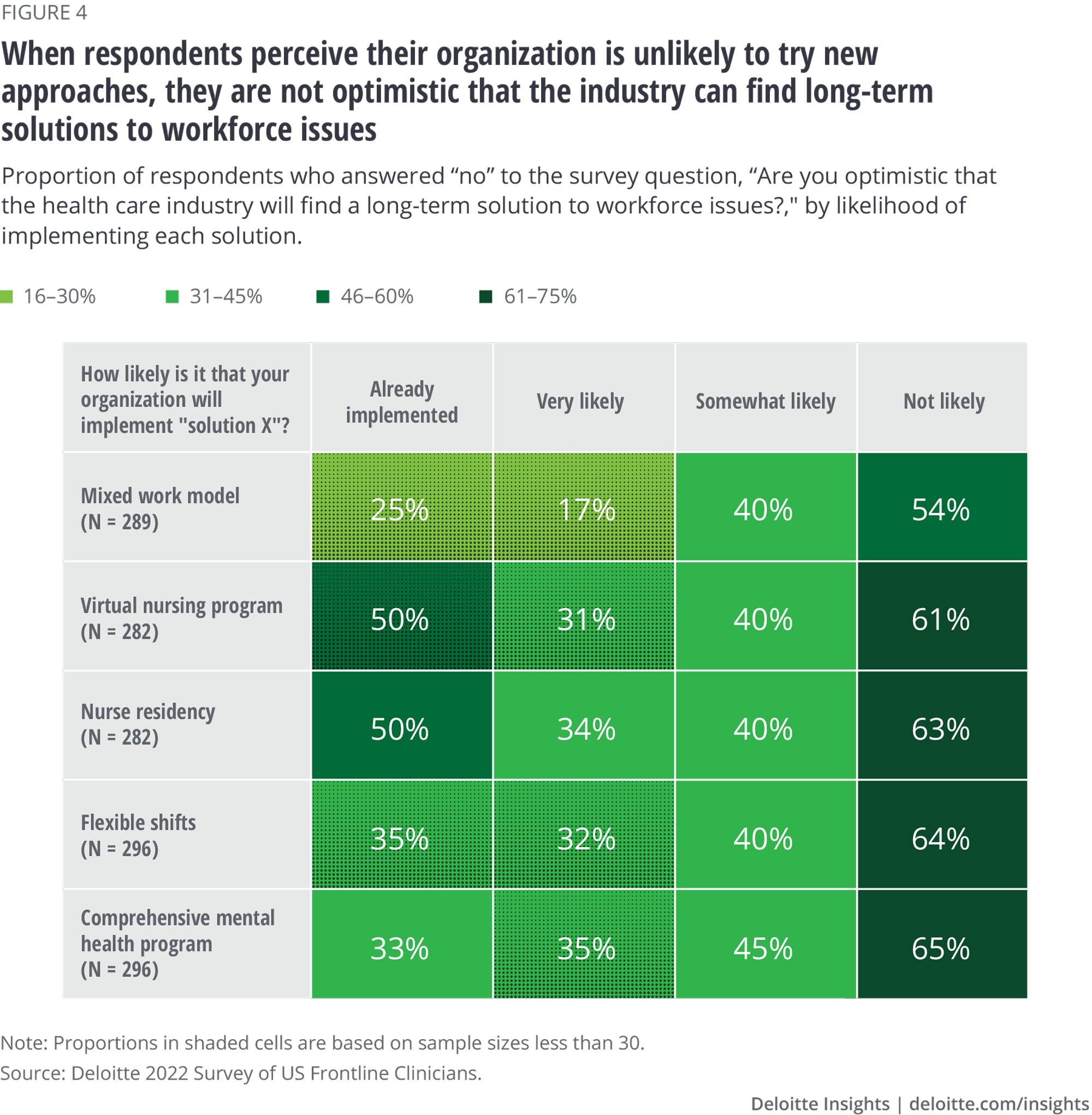
Our findings give us hope: Even though frontline clinicians are largely pessimistic that the industry can find a long-term solution, the outlook is significantly brighter in workplaces where respondents perceive the appetite to implement innovative solutions. We interpret this as a sign that the industry is capable of innovating and can garner the goodwill to commit to long-term strategies to solve the talent emergency and avert future crises.
Introduction: The clinician shortage is industrywide
Today, health care organizations are facing an industrywide talent emergency due to unprecedented levels of burnout and attrition that led to shortages of frontline clinicians (and health workers more generally).4 Our survey results paint a dire picture: About half (46%) of the clinicians reported high levels of burnout, 35% said their burnout is modest, and only 19% reported no or minimal burnout.
For health care organizations, the shortage of health workers is a complex problem, with several underlying causes. Research shows that numerous organizational and systemic factors—such as work design, culture, workforce supply, and policy—are responsible for frustration, dissatisfaction, and burnout.5
Clinician shortages are a strain against organizations’ missions to serve patients and the community. After years of steady decline, the incidence of health care–associated infections significantly increased in 2020, according to CDC analysis. Researchers cite staffing shortages and high caseloads as some of the reasons for this increase.6 Several other recent studies point to a link between workforce shortfalls and increases in patient safety events.7 Researchers have long warned of burnout and staffing shortages as threats to high quality and safe care.8 In our survey, almost all clinicians are concerned that health care worker burnout (98%) and shortages (99%) can result in decreased quality of care in their communities.
The public is also increasingly aware of the problem and concerned about how it could impact their health. The Deloitte 2022 Survey of US Health Care Consumers found that four in five (82%) consumers are aware of the health care worker shortage. And about seven in 10 are concerned that the worker shortage may affect their own health, and that of their families (67%) and communities (69%).
As more burned-out clinicians leave their organizations or health care altogether, the industry has responded with tried-and-true tactics like leveraging existing workers to work overtime and using staffing agencies to fill in gaps. However, we’re beginning to see the limitations of this old playbook. Health systems are incurring large losses due to the high cost of contract labor, which grew to 11% of total labor expenses in 2022 from 2% in 2019.9 Furthermore, compensation disparities between temporary and permanent staff and the constant need to educate temporary staff deepen tensions and burnout among permanent staff, prompting them to turn to contract assignments.
It's time to acknowledge that old tools have outlived their usefulness and we need creative solutions to solve the issue at hand and avert future crises.
Recommendations to address the clinician shortage
Our research shows that to address the talent emergency, health systems should fundamentally transform the way they deliver care. This calls for new models for how clinicians work, who they work with, and where they work. While redesigning the work should be at the center, these transformation efforts cannot succeed without ongoing investments in people and rebuilding trust in leadership.
Reimagine care delivery and redesign the work
Truly addressing burnout and improving clinician well-being isn’t easy, according to our interviewed experts, and likely requires a complete care model transformation and job redesign.
Invest in technology to give time back to clinicians
Workflow inefficiencies place a heavy cognitive burden on clinicians. Currently, numerous unnecessary and low-value tasks in clinicians’ day-to-day work take time away from the clinical work. When asked what is one thing that clinicians currently do in their job that has minimal clinical value and could be eliminated, activities to satisfy administrative requirements (32%) and work that could be done by others or automated (20%) were the top two low-value tasks they identified. For physicians, computer-related and insurance-related tasks were the top low-value activities after administrative work. Getting rid of these low-value tasks could offer some quick fixes for optimizing workflows and reducing burnout. For example, the AMA STEPS Forward™ module10 offers a standardized organizational process to identify and eliminate such tasks.11
Given how much time clinicians spend updating EHRs every day, EHR optimization is a critical lever to reduce the burden on clinicians. Organizations can start with EHR analytics to identify tasks that consume large amounts of time across the board and identify areas to reduce clicks and time spent in the EHR. One option is to improve in-basket management. A large medical group eliminated 1.7 million clicks in a year by automatically transferring notifications of admission, discharge, and transfer from physicians' inboxes to case managers. Additionally, use of widescreen monitors made it easier for physicians to keep multiple windows open, further reducing the number of clicks.12

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}