Reimagining health care delivery has been saved

Perspectives
Reimagining health care delivery
Platforms propelling new care models
The health care industry stands at a pivotal juncture, grappling with escalating costs, labor shortages, and a dissatisfied consumer base. The conventional paradigms governing health care delivery and financing are being shattered, requiring a fundamental change—inspired by platforms and personalization. Explore how the unbundling and rebundling of health care services can help align to the growing demands of customers.
Leveraging platforms to accelerate health care personalization
Much like the transformative shifts observed in industries such as television, banking, and transportation, the health system is due to undergo massive changes. This likely requires a fundamental unbundling and rebundling of the health value chain in new ways; unbundling—unpacking a provider’s full range of services; and rebundling—identifying customized options based on a patient’s medical needs.
This shift is essential to not only align with the evolving demands of consumers, but also to help yield desired outcomes and establish a sustainable framework for potentially substantial cost reduction. In our 2021 paper The power of networked ecosystems: How platforms can be a force-multiplier in health, we demonstrated how new business models like platforms can cocreate goods and services, enable wider customer reach, provide access to new capabilities, and help increase revenue.
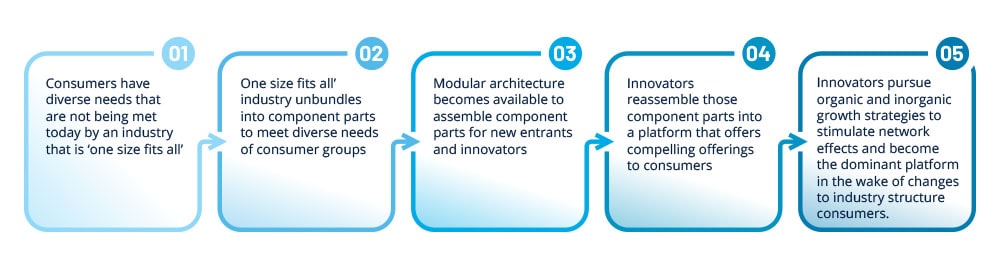
Figure 1: Platform business journey
But how can established players—the incumbents—benefit from their core while preparing for the newly emerging market?
From pipelines to platforms: How empowered consumers have driven unbundling and rebundling—and what it means for health care
What is the impact of "empowered consumers" on business? Understanding it is crucial, because when they emerge, entire industries are often rewired to satisfy their idiosyncratic needs.
Digital technologies have enabled the unbundling of information and content and, the formation of new bundles to create value for the consumer—rebundling. The same change is taking place in health care. Companies that can cater or "bundle" their products or services to fragmented communities have prospered. Consider Amazon with its "people like you" algorithms, or Airbnb with homes that fit your aesthetic.
COVID-19 accelerated the change of existing care models that were "one size fits all" (e.g., primary care). These newer care models consider the needs of underrepresented populations and reimagined the services to provide them to all populations. However, health care is different in that the consumer is not the sole buyer of health services. Thus, platform businesses in health should align to the dynamics of the industry.
Enter 'reassembly'—the formation of partnerships between the innovators who have customer loyalty and digitally enabled products, and the incumbents who have scale and expertise in the delivery of complex care.
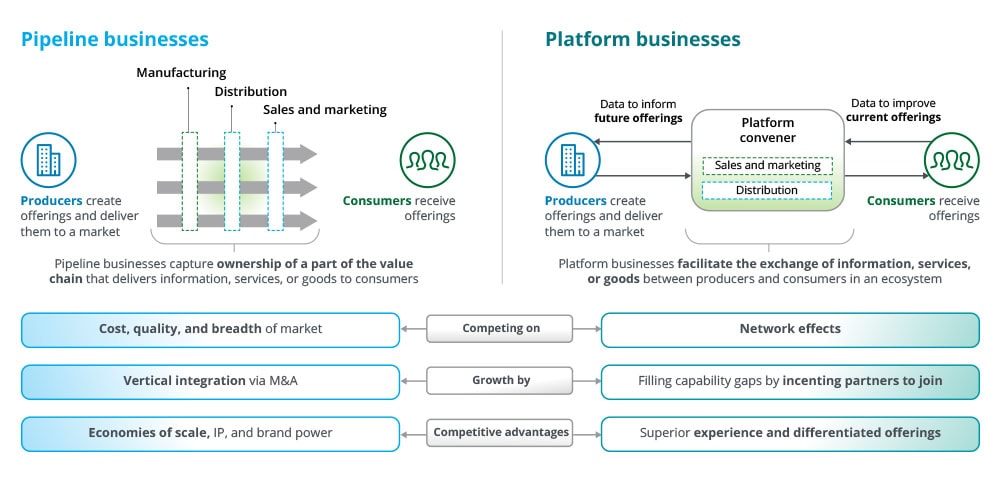
Similar to what we've seen in media and retail, the reassembly of the health care industry is being catalyzed by a different business model: the platform business. But historically, companies have been organized as pipeline business models, delivering value in a linear fashion from the production of a good or service to the delivery of that good or service to the consumer. Pipelines seek to own all parts of the value chain. But in contrast, a platform business can be non-linear; it has the infrastructure to facilitate the exchange of information, services, or goods (figure 2).
Figure 2: Platform business models are rewiring the value chain
Can primary care become the platform to serve up improved health care?
Primary care needs an overhaul to align to the demands of diverse communities
Health systems have historically employed a one-size-fits-all care model, using the same care model for all patients regardless of population. But literature demonstrates that the availability and quality of primary care is associated with higher health status; every additional 10 primary care physicians (PCPs) were linked to an increased life expectancy of 51.5 days.1
Different components of primary care and how it can be unbundled and rebundled to create value for consumers:
- Population: Certain communities have care needs specific to their demographics (e.g., senior primary care, women’s care).
- Service mix: Much of primary care can be provided as discrete services (e.g., urgent care, chronic condition management).
- Service modality: There is not a single ideal modality for care. New care models should align to consumers where they are and could consider using underutilized labor pools (e.g., emergency medical technicians, or EMTs, in the home for seniors).
- Business model: The delivery of primary care services can occur through various business models including B2C, B2B, B2B2C, and B2C2B.
Who will be on the podium?
The race to build platforms in health care
A platform mindset in health means:
- Patients are guided to different sites of care (e.g., virtual, physical, home) and matched with different care programs.
- Providers are enabled by plug-and-play tools and analytics to support the transition to value-based care (VBC).
- Advanced analytics can unlock powerful learnings and identify when patients deviate and may be at risk.
- Most importantly, the platform won’t seek to own everything but instead own the infrastructure for other partners to transact on.
What’s required?
Platforms need a plug-and-play technology architecture
Traditional companies are often constrained by scarce resources, while platform companies are typically better positioned to amplify their potential by convening an ecosystem of partners.
This calls for a significant adjustment in technology architecture. The architecture should include the following features:
- Experience layer
- Analytics layer
- Interoperability and orchestration layer
- Cloud-based layer
Fundamentally, a platform businesses partner with an ecosystem of innovators to help achieve network effects, and this is powered by a plug-and-play infrastructure to allow integration into diverse partner tech stacks.
A plug-and-play platform should have the following components:
- A recommendation engine to match the patient with the appropriate innovator; analytics to identify unmet needs for consumer/patient
- A longitudinal health record that spans clinical, claims, social determinants of health (SDOH), consumer-mediated
- A marketing engine that executes enrollment campaigns across modalities
- A deep level of integration based on consistent data standards and architectural patterns (e.g., bidirectional, software developments kits)
- Transparency of experience in connected workflows (e.g. provider can see if their delegated patients are actively engaging with their digital therapeutic)
- A feedback loop and learning framework that continuously refines campaigns, actions, pathways, based on outcomes achieved
A stepwise approach to a plug-and-play architecture is possible and requires careful calibration of the partners and use cases (areas for focus) to help generate adoption and quick wins that build support for catalyzing the flywheel effect. User adoption is critical to unlock the ambitions of a platform business.
What does health care want to be next?
The reassembly of care poses existential questions for the industry
Companies across the industry—plans, providers, medical device, and health tech companies—should seek to answer questions to help define their role in a network of ecosystems.
- What does it mean when a payvider, consumer tech company, or retailer is consulted on where patients go for their care?
- Is there a tipping point where a nontraditional health care entrant becomes more trusted after so many convenient interactions?
- When patients are guided to different modalities, what happens to traditional inpatient modalities with high fixed costs?
- How can health systems respond to disruption posed by payviders, consumer tech companies, and retailers? What happens to the health systems’ profit pools?
- What does it mean for the economics of care as more payviders embrace VBC?
- How can the increasing demands of personalization in care be balanced with the need for scale?
Answers to these questions will require experimentation. One can test whether their offering is viable in an ecosystem through a curated set of partners called a minimal viable ecosystem. A concerted strategy, a reliable set of partners, and a deliberate technology stack can help secure one's positioning in the ongoing reassembly of health care.
Endnote:
1Beth Duff-Brown, "More primary care physicians leads to longer life spans," Stanford Medicine News Center, May 18, 2019.
Contacts
Neal Batra |
Simon Gisby |
Jen Radin |
Jeanette Yung |
Boris Kheyn-Kheyfets |
Recommendations

Future of Health™
Listen in and prepare to lead in the future of health care

The power of digital health care ecosystems
Embracing platforms is giving rise to new business models